-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(2): 417-420
doi:10.5923/j.ajmms.20261602.06
Received: Jan. 7, 2026; Accepted: Jan. 29, 2026; Published: Feb. 3, 2026

Intergroup Specific Features of Lipid and Renal Parameters in Patients with Ischemic Heart Disease
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLTulaboeva G. M.1, Sobirova Sh. S.2
1Center for the Development of Professional Qualification of Medical Workers, Tashkent, Uzbekistan
2Bukhara State Medical Institute, Bukhara, Uzbekistan
Correspondence to: Sobirova Sh. S., Bukhara State Medical Institute, Bukhara, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The study evaluated lipid and renal function parameters in 125 elderly patients with ischemic heart disease (IHD). Patients were divided into two groups: Group 1 – IHD with arrhythmia, Group 2 – IHD without arrhythmia. Group 1 showed higher total cholesterol, LDL-C, triglycerides, urea, and creatinine, and lower HDL-C and GFR (p<0.001). Strong inverse correlations were found between GFR and LDL-C (ρ≈−0.45), and between GFR and microalbuminuria (ρ≈−0.65). Dyslipidemia and renal impairment were identified as major contributors to the cardio-renal-metabolic continuum in IHD. Integrated monitoring of these indicators is essential for risk stratification and improving prognosis.
Keywords: Ischemic heart disease, Lipid profile, Renal function, GFR, Arrhythmia, Microalbuminuria, Cardio-renal syndrome
Cite this paper: Tulaboeva G. M., Sobirova Sh. S., Intergroup Specific Features of Lipid and Renal Parameters in Patients with Ischemic Heart Disease, American Journal of Medicine and Medical Sciences, Vol. 16 No. 2, 2026, pp. 417-420. doi: 10.5923/j.ajmms.20261602.06.
Article Outline
1. Introduction
- Ischemic heart disease (IHD) remains the leading cause of morbidity and mortality worldwide, especially among elderly populations [1,2]. The coexistence of metabolic and renal dysfunction in these patients contributes to disease progression and worsens prognosis [3]. Lipid metabolism disorders elevated total cholesterol, low-density lipoprotein cholesterol (LDL-C), and triglycerides, together with reduced high-density lipoprotein cholesterol (HDL-C) play a pivotal role in atherogenesis and vascular remodeling [4,5].Meanwhile, renal impairment in IHD patients, manifested by reduced glomerular filtration rate (GFR) and elevated serum creatinine or urea levels, often reflects systemic endothelial dysfunction and neurohumoral activation [6]. The cardio-renal interaction leads to mutual deterioration of heart and kidney function, forming a “vicious circle” that aggravates metabolic imbalance [7,8].Comprehensive assessment of both lipid and renal parameters therefore provides essential insights into cardiovascular risk stratification and therapeutic optimization [9]. Comparative analysis between IHD patients with and without arrhythmia or renal comorbidity can reveal specific metabolic-renal interrelations that underlie disease severity and quality-of-life outcomes [10].The purpose of the study was to evaluate and compare the intergroup differences in lipid metabolism and renal function indicators among patients with ischemic heart disease (IHD), and to determine the relationship between dyslipidemia, renal impairment, and clinical disease severity. The study sought to identify diagnostic and prognostic significance of these parameters for improving risk stratification and therapeutic management in elderly patients with IHD.
2. Material and Methods
- The study was conducted at the Cardiology Department of the Bukhara Regional Branch of the Republican Specialized Scientific and Practical Medical Center for Internal Diseases. A total of 125 elderly patients aged 59 to 73 years (mean age 66.0±4.4) were enrolled. Patients were divided into two groups according to the presence of life-threatening arrhythmias: Group 1 (n = 65) IHD with arrhythmia; Group 2 (n = 60) IHD without arrhythmia.The diagnosis of ischemic heart disease (IHD) was established based on clinical findings, electrocardiography (ECG), and echocardiography (EchoCG) data in accordance with the recommendations of the European Society of Cardiology (ESC, 2019) and the Russian Society of Cardiology (RSC, 2020).Quality of life was assessed using the Minnesota Living with Heart Failure Questionnaire (MLHFQ). Instrumental examinations included ECG, EchoCG, 24-hour blood pressure monitoring (ABPM), and renal artery Doppler ultrasonography.Laboratory tests included measurements of serum creatinine, urea, lipid profile, HbA1c, and C-reactive protein (CRP) levels. The glomerular filtration rate (GFR) was calculated using the CKD-EPI formula.Statistical analysis was performed using Student’s t-test, Mann–Whitney U test, and χ² test, with a significance level of p<0.05 considered statistically significant.
3. Results and Analyses
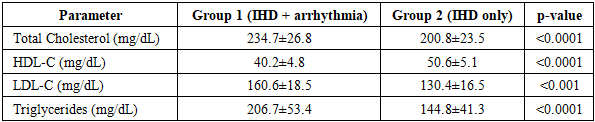
- In this study, lipid metabolism was compared between Group 1 (IHD + arrhythmia, n = 65) and Group 2 (IHD without arrhythmia, n = 60). Mean total cholesterol was significantly higher in Group 1 (234.7±26.8 mg/dL) than in Group 2 (200.8±23.5 mg/dL; p<0.0001). High-density lipoprotein cholesterol (HDL-C) levels were lower in Group 1 (40.2±4.8 mg/dL) compared with Group 2 (50.6±5.1 mg/dL; p<0.0001). Low-density lipoprotein cholesterol (LDL-C) was markedly higher in Group 1 (160.6±18.5 mg/dL) than in Group 2 (130.4±16.5 mg/dL; p<0.001). Triglyceride levels were also elevated in Group 1 (206.7±53.4 mg/dL) versus Group 2 (144.8±41.3 mg/dL; p<0.0001).These findings indicate a pronounced atherogenic lipid pattern in patients with life-threatening arrhythmias, confirming higher cardiovascular risk (table 1).
|
|
|
|
4. Discussion
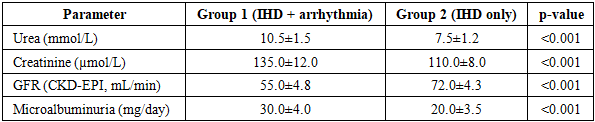
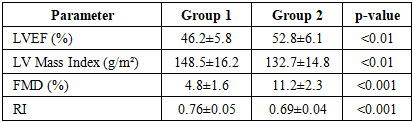
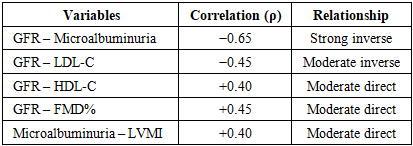
- The findings of this study clearly demonstrate that patients with ischemic heart disease (IHD) complicated by life-threatening arrhythmias exhibit significantly more severe metabolic and renal dysfunctions compared to those with isolated IHD. The observed elevation of total cholesterol, LDL-C, and triglycerides, along with decreased HDL-C levels, confirms a pronounced atherogenic lipid profile that contributes to vascular remodeling and a higher risk of adverse cardiac events [4,5,9]. These results align with previous research emphasizing the pivotal role of dyslipidemia in promoting endothelial damage and myocardial ischemia [1,2,9].Renal impairment was another distinct feature in patients with combined IHD and arrhythmia, as evidenced by elevated serum creatinine and urea, reduced glomerular filtration rate (GFR), and increased microalbuminuria. These alterations reflect the development of cardiorenal syndrome, in which chronic myocardial ischemia, reduced cardiac output, and arrhythmia-induced hemodynamic instability lead to renal hypoperfusion and nephron damage [3,7,8,13,14]. The data are consistent with reports showing that renal dysfunction serves both as a consequence and an aggravating factor of cardiovascular disease, particularly in elderly populations [6,15].The strong inverse correlations found between GFR and LDL-C, as well as between GFR and microalbuminuria, suggest that worsening renal filtration parallels dyslipidemia progression. Conversely, a positive relationship between GFR and HDL-C indicates that preserved renal function is associated with favorable lipid profiles [4,5,16]. These interactions highlight the bidirectional link between lipid metabolism and renal function, forming a metabolic feedback loop that accelerates atherosclerosis and cardiac remodeling.Moreover, the reduction in flow-mediated dilation (FMD %) observed in arrhythmic patients points to endothelial dysfunction, which correlated inversely with microalbuminuria and LDL-C. This relationship reinforces the view that oxidative stress, inflammation, and impaired nitric oxide bioavailability jointly drive both renal and vascular deterioration [7,8,17].Echocardiographic findings of lower ejection fraction and increased left ventricular mass index (LVMI) in arrhythmic patients further support the concept of structural myocardial remodeling secondary to chronic ischemia and metabolic derangements. Prior studies have shown that renal dysfunction and dyslipidemia promote ventricular hypertrophy through neurohumoral activation and increased afterload [10,13,16].Overall, these results confirm the existence of a cardio-renal-metabolic continuum, in which dyslipidemia, renal impairment, and endothelial dysfunction act synergistically to worsen prognosis in elderly IHD patients [11,12,18]. Early detection and correction of lipid abnormalities, monitoring of renal function, and endothelial protection represent essential components of an integrated therapeutic strategy. Comprehensive rehabilitation and individualized management, as emphasized in recent guidelines, can substantially improve quality of life and long-term survival [17,19].
5. Conclusions
- This study demonstrated that patients with ischemic heart disease (IHD) complicated by life-threatening arrhythmias have significantly higher levels of total cholesterol, LDL-C, triglycerides, serum creatinine, and urea, as well as reduced HDL-C and glomerular filtration rate (GFR), compared to those with isolated IHD. These findings confirm the coexistence of dyslipidemia and renal dysfunction as integral components of the cardio-renal-metabolic continuum.The observed inverse correlations between GFR and LDL-C or microalbuminuria, along with the positive association between HDL-C and endothelial function (FMD%), indicate that lipid and renal markers jointly determine disease progression and cardiovascular risk. Structural and functional cardiac alterations, such as reduced ejection fraction and increased left ventricular mass index, further underline the interplay between metabolic and hemodynamic factors.Comprehensive evaluation of lipid and renal parameters should therefore be considered a key diagnostic and prognostic approach in elderly IHD patients. Early correction of dyslipidemia, preservation of renal perfusion, and endothelial protection may improve clinical outcomes, reduce complications, and enhance quality of life.