Akramova Khursandoy Abdumalikovna1, Bayjanova Gulnoza Jumanazar qizi2, Kilicheva Tukhtagul Abdullaevna2, Madrahimov Polvon Masharibovich2, Davletova Fotima Otabekovna2, Artikova Gulmira Zafarovna3, Sobirova Nigora Ahmedovna3, Ibragimova Shoxista Mamatsodiqovna3
1Doctor of Medical Sciences, Associate Professor, Tashkent State Medical University, Tashkent, Uzbekistan
2Assistant, Urgench State Medical Institute, Urganch, Uzbekistan
3Neonatologist, Khorezm Branch of the Republican Specialized Scientific and Practical Medical Center of Mother and Child Health, Urganch, Uzbekistan
Correspondence to: Akramova Khursandoy Abdumalikovna, Doctor of Medical Sciences, Associate Professor, Tashkent State Medical University, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Functional bowel disorders (FBD) in young children are one of the most common problems in pediatric practice. Their course is often accompanied by alterations in gastrointestinal motility, abdominal pain syndrome, bowel movement disorders, and a decreased quality of life in the child. In recent years, particular attention has been given to the combination of functional gastrointestinal disorders (FGIDs) with anemic syndrome, which is one of the most prevalent pediatric pathologies and is characterized by a high prevalence rate. The presence of anemia in young children against the background of functional intestinal disorders worsens the clinical course of the disease, affects nutritional status, and impairs the rate of physical and psychomotor development.
Keywords:
Disfunction, Anamnesis, Anemia, Breastfeeding, Diarrhea
Cite this paper: Akramova Khursandoy Abdumalikovna, Bayjanova Gulnoza Jumanazar qizi, Kilicheva Tukhtagul Abdullaevna, Madrahimov Polvon Masharibovich, Davletova Fotima Otabekovna, Artikova Gulmira Zafarovna, Sobirova Nigora Ahmedovna, Ibragimova Shoxista Mamatsodiqovna, The Influence of Anamnestic Factors on the Manifestations of Various Forms of Functional Intestinal Disorders in Children with Anemia, American Journal of Medicine and Medical Sciences, Vol. 16 No. 2, 2026, pp. 410-413. doi: 10.5923/j.ajmms.20261602.04.
1. Introduction
Data analysis indicates that children with anemia and functional intestinal disorders (FID) more frequently develop unfavorable disease courses associated with a high risk of recurrence and complications [1,2,3,4]. The patient history in the study by Ibragimov A.I. across various patient categories—including information on dietary patterns, previous infections, and comorbid somatic conditions—allows for the identification of risk groups and the clarification of the mechanisms underlying pathological manifestations.The utilization of clinical and anamnestic data in a physician's scientific and practical activities serves as an essential tool for early detection of disorders, optimization of diagnostic tactics, and individualization of therapy. It is emphasized that a comprehensive approach to managing children with FID in the context of anemia ensures not only symptom correction but also the prevention of further progression of functional digestive system disorders. This, in turn, facilitates the selection of more effective strategies for diagnosis, treatment, and the prevention of complications. Thus, the study of anamnestic risk factors for FID in children with anemic syndrome is a pressing task in modern pediatrics, aimed at improving the quality of medical care and reducing the incidence of adverse outcomes [5].The Aim of the research. To evaluate the influence of anamnestic factors on the manifestations of various forms of functional intestinal disorders in young children with anemia.
2. Materials and Methods
The study involved 164 young children (aged 1 to 3 years). The primary group consisted of 144 patients with FID diagnosed against the background of anemia of varying severity (mild, moderate, and severe forms). The control group included 20 children with anemia without signs of FID. The classification of functional intestinal disorders was carried out according to the ICD-10 criteria. Antenatal and perinatal histories were collected, and a comprehensive laboratory examination was performed, including biochemical blood analysis to determine levels of total protein, calcium, iron, ferritin, vitamin B₁₂, and vitamin D. This allowed for the identification of concomitant deficiency states associated with anemic syndrome and impaired intestinal function.According to our data, the gender distribution in the primary group was as follows: 86 boys (59.7%) and 58 girls (40.2%). In the control group, the gender distribution was equal, consisting of 10 boys (50%) and 10 girls (50%).
3. Results and Discussion
Among the 144 children with functional intestinal disorders, the largest proportion consisted of cases of unspecified functional intestinal disorders (ICD-10: K59.9), observed in 76 patients (52.7%). This underscores their leading position in the structure of these diseases among young children. Functional diarrhea (K59.1) was diagnosed in 41 children (28.0%), while functional constipation (K59.0) was noted in 27 children (19.3%) (Diagram 1).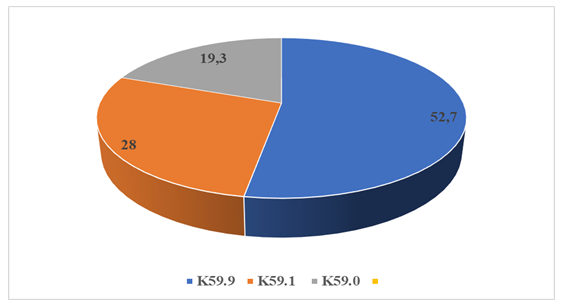 | Diagram 1. Distribution of children in the primary group by types of functional intestinal disorders, % |
Age distribution analysis revealed that the predominant majority of the subjects were children in their first year of life, accounting for 107 patients (74.3%). The results of the mothers' obstetric history in the study groups showed that among the children in the primary group (n=144) with FID of various nosological structures against the background of anemia, there were significant differences related to the order of pregnancy and the characteristics of delivery. Specifically, in cases of grade I anemia (n=36), 36.1% (n=13) of the children were born from the first pregnancy; in grade II (n=93), this figure was 22.5% (n=21), and in grade III (n=17), it was 29.4% (n=5). Children born from the second pregnancy accounted for 15.0% (n=14) in grade I anemia, 56.9% (n=53) in grade II, and 4.2% (n=4) in grade III. An increase in the frequency of grade II and III anemia (19.3% and 29.4%, respectively) was observed in children born from the third and subsequent pregnancies. The statistical significance of the differences was confirmed (p≤0.001). In the primary group of children with FID (K59.9) associated with grade I anemia, there was no significant difference between physiological delivery and cesarean section (5.5–6.5%). However, in cases of grade II anemia, the proportion of cesarean sections increased significantly to 43.4%. Mothers of children in this group more frequently exhibited chronic diseases (65.7%) and pregnancy complications, predominantly gestational toxicosis (26.3%). In grade III anemia, a high incidence of maternal anemia (10.5%) and obstetric complications, including gestational toxicosis (7.8%), was observed. Similar trends were identified in children with FID (K59.1, n=41): in cases of grade I anemia, cesarean section was noted in 17.0% of cases, and maternal anemia in 12.9%. In grade II, the combination of unfavorable factors was more pronounced: cesarean section accounted for 36.5%, chronic diseases for 24.3%, and gestational toxicosis (gestosis) for 24.3%. In grade III, a significant proportion of maternal pathologies persisted (chronic diseases – 9.7%). In the group of children with FID (K59.0, n=27) and grade I anemia, maternal anemia (14.8%), gestosis (29.6%), and chronic diseases (33.3%) were more frequently recorded. In grade II, the most prominent risk factors were maternal chronic diseases (37.0%) and gestosis (37.0%), confirming their role in the pathogenesis of FID. In grade III anemia, the trend toward a high frequency of chronic pathology (18.5%) and obstetric complications also remained consistent. In the control group (n=20), despite the absence of FID, a comparable trend was observed. In cases of grade I anemia, the frequencies of physiological delivery and operative delivery (cesarean section) were 35.0% each, while maternal chronic diseases were noted in 30.0% of women. In grade II anemia, cesarean section accounted for 15.0%, chronic diseases for 35.0%, and gestational toxicosis for 20.0%. In the subgroup of children with grade III anemia, a high incidence of complicated labor (30.0%), maternal anemia (20.0%), and chronic pathology (30.0%) was recorded. The high frequency of cesarean sections in grade II and III anemia may be associated with obstetric complications requiring surgical intervention, which, in turn, influences the formation of the newborn's microbiota. It is well established that children born via cesarean section carry a higher risk of functional intestinal disorders due to the lack of contact with maternal vaginal flora and delayed intestinal colonization by beneficial microorganisms. The presence of maternal chronic diseases, as well as gestational toxicosis and anemia during pregnancy, creates conditions for chronic intrauterine hypoxia, fetal nutritional impairment, and delayed functional development. Taken together, these factors may act as triggers for the development of anemia in the child and the onset of FID in the postnatal period.Breastfeeding is the optimal form of nutrition for children in their first years of life and exerts a comprehensive influence on the child's growth, development, and long-term health [6]. Breast milk contains all essential nutrients, immunologically active components, and bifidogenic factors that cannot be replicated in artificial formulas [7]. Breastfeeding is of particular importance for the formation of the intestinal microbiota [8]. A balanced microbiota in early childhood promotes the proper development of the immune system and metabolic processes, while reducing the likelihood of developing chronic diseases in the future [9].Analysis of feeding patterns revealed specific regularities among children with FID and varying degrees of anemia, reflecting the role of early nutrition in the development of pathological conditions. In the primary FID group (K59.9, n=76), infants with grade I anemia (n=13) were predominantly breastfed (11.8%), while only 5.2% were formula-fed. In grade II anemia (n=55), breastfeeding remained dominant (43.4%), although a significant proportion of mixed and formula feeding was noted (14.4% each). In grade III anemia (n=8), a relative balance between feeding types was observed: 10.5% of children were breastfed, 2.6% were formula-fed, and 3.9% received mixed feeding. This indicates that more severe anemia is associated with a higher dependence on mixed and formula feeding (Diagram 2).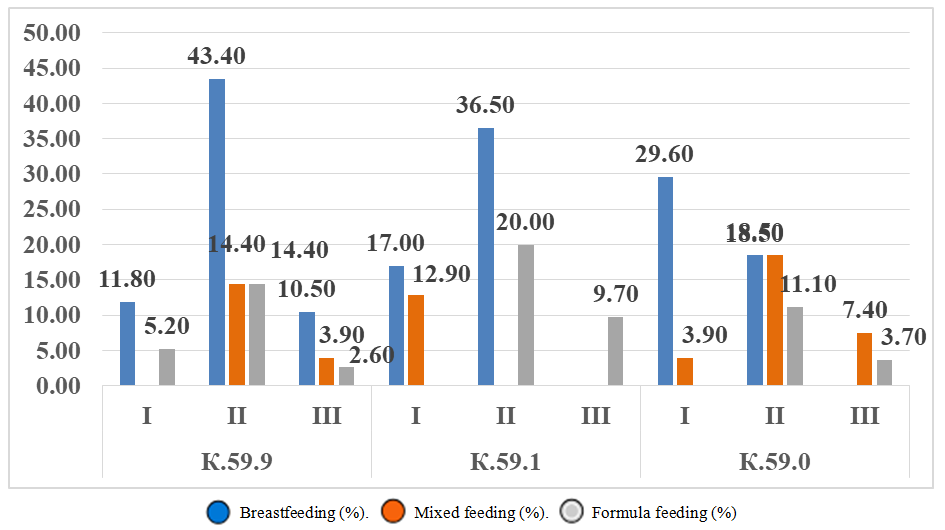 | Diagram 2. Feeding patterns in children of the primary group (%) |
In the FID group (K59.1, n=41), among children with grade I anemia (n=12), the proportion of breastfeeding was 17.0%, while mixed feeding accounted for 12.9%, highlighting a decline in the role of exclusive breastfeeding. In grade II anemia (n=25), breastfeeding was predominant (36.5%); however, in 20.0% of cases, children were formula-fed, indicating its possible role in the progression of disorders. In children with grade III anemia (n=4), exclusive formula feeding dominated (9.7%), which can be considered one of the risk factors for a more severe clinical course.In the FID group (K59.0, n=27), among children with grade I anemia (n=11), 29.6% were breastfed, while mixed feeding accounted for 3.9%. In grade II anemia (n=13), the proportion of breastfeeding decreased (18.5%), while the shares of mixed and formula feeding increased (18.5% and 11.1%, respectively; p<0.05). In grade III anemia (n=5), a pronounced trend toward mixed and formula feeding was observed (7.4% and 3.7%, respectively). Summarizing the research results, it can be concluded that the feeding patterns of children with FID exhibit specific characteristics depending on the nosological group. In the K59.9 group, breastfeeding remains dominant (21.90 ± 10.0%). Despite relatively high breastfeeding rates, the shares of mixed feeding (6.10 ± 4.4%) and formula feeding (7.40 ± 3.9%) remain notable, which may indicate the insufficiency of exclusive breastfeeding against the background of varying degrees of anemia. In the K59.1 group, the level of natural feeding is lower (17.83 ± 10.8%), with a significant proportion of formula feeding (9.90 ± 5.8%). This highlights the possible influence of an early transition to artificial formulas on the development of more pronounced functional intestinal disorders and varying degrees of anemia. In the K59.0 group, a relatively low level of natural feeding is observed (16.03 ± 8.9%), with a noticeable predominance of the mixed feeding variant (9.93 ± 4.3%). It is likely that the combination of breast milk and formula reflects the compensatory nature of feeding, but it may simultaneously reduce the preventive effect of breastfeeding. Analysis of the control group by feeding type depending on the severity of anemia showed that among children with grade I anemia (n=3), 42.8% were breastfed, while formula and mixed feeding occurred equally (28.5% each). In grade II anemia, 3 children (42.8%) were breastfed, and 4 (57.1%) were formula-fed. In grade III anemia, 2 children (33.3%) were breastfed, and 4 (66.7%) were formula-fed. Notably, the control group was characterized by a predominance of formula-fed children in the grade II and III anemia subgroups (57.1% and 66.7%, respectively; p<0.05). The mean values by feeding type were 39.6 ± 3.17% for breastfeeding, while the highest percentage was observed for formula feeding (50.8 ± 11.48%), and mixed feeding accounted for 9.5 ± 9.5%.The study revealed a high frequency of comorbidities associated with anemia. In the group with unspecified FID (K59.9) and grade I anemia, grade 1–2 rickets was observed in 10 patients (13.1%); in grade II anemia, it was found in 47 children (61.8%), and in grade III anemia, in 8 children (10.5%). Atopic dermatitis was also recorded in this category of patients: in grade I anemia, it affected 4 children (5.2%); in grade II, 18 children (23.6%); and in severe anemia, 2 patients (2.6%).In functional diarrhea (K59.1), the association with comorbidities was also pronounced. Among children with grade I anemia, rickets was identified in 10 cases (24.3%), while in moderate (grade II) anemia, it was found in 22 children (53.6%). At the same time, in severe (grade III) anemia, it was observed in 2 children (4.8%). Atopic dermatitis was also identified in these patients: in grade I anemia, in 5 children (12.2%); in grade II, in 14 children (34.1%); and in severe anemia, in 1 patient (2.4%). In the group of children with functional constipation (K59.0), comorbid rickets was observed in 9 cases (33.3%) among those with grade I anemia, and in 10 children (37.0%) with moderate (grade II) anemia. At the same time, in severe (grade III) anemia, it was recorded in 1 child (3.7%). Atopic dermatitis was also identified in these patients: in grade I anemia, in 8 children (29.6%); in grade II, in 5 children (18.5%); and in severe anemia, in 1 patient (3.7%).In the control group, rickets was identified equally in children with grade I and grade II anemia, occurring in 5 cases (25.0%) each, while in severe anemia, it was found in 2 children (10.0%). At the same time, atopic dermatitis was observed in these patients as follows: in grade I anemia, in 2 children (10.0%), and in grade II and III anemia, it occurred equally in 3 children (15.0%) each.
4. Conclusions
The findings indicate that ante- and perinatal risk factors play a pivotal role in the development of FID in children with anemia. Among these factors, cesarean section, maternal chronic diseases, and complicated pregnancy are of the greatest significance. These circumstances necessitate the implementation of comprehensive preventive measures and rigorous clinical follow-up for children in high-risk groups. Furthermore, the results of the study highlight gender differences, suggesting that boys are more susceptible to the development of functional intestinal disorders in the presence of anemia.
References
| [1] | Dmitrieva Y.A, Zakharova I.N. The role of nutrition in the postnatal development of the child's gastrointestinal tract. Trudnyy Patsiyent (Difficult Patient). 2020; 18(1-2): 47-52. (In Russ). |
| [2] | Evstigneev I.V. Immunological research methods in the diagnosis of diseases of the large intestine. Klinicheskaya immunologiya, allergologiya, infektologiya (Clinical Immunology, Allergology, Infectology). 2012; (1-2): 22-32. (In Russ). |
| [3] | Erofeev N.P, Radchenko V.G, Seliverstov P.V. Clinical physiology of the colon. Mechanisms of action of short-chain fatty acids in health and disease. St. Petersburg: Forte Print; 2012. 56 p. (In Russ). |
| [4] | Bayjanova G.J. Dysfunctional intestinal disorders in young children in the Khorezm region. Vestnik nauki i obrazovaniya (Bulletin of Science and Education). 2024. |
| [5] | Bayjanova G.J, Akramova Kh.A. Clinical features of functional disorders of the gastrointestinal tract among young children. Evraziyskiy vestnik pediatrii (Eurasian Bulletin of Pediatrics). 2024; 4. |
| [6] | Erpuleva Y.V. Modern organization of nutritional support in children with surgical pathology. Rossiyskiy vestnik detskoy khirurgii, anesteziologii i reanimatologii (Russian Journal of Pediatric Surgery, Anesthesia and Intensive Care). 2019; 9(3): 102-109. (In Russ). |
| [7] | Zakharova I.N. Clinical possibilities of multiprobiotics in pediatric practice. Effektivnaya farmakoterapiya (Effective Pharmacotherapy). 2016; (40): 32-38. (In Russ). |
| [8] | Zakharova I.N, Sugyan N.G, Ardatskaya M.D. Metabolic activity of intestinal microflora in infants with digestive disorders. Effektivnaya farmakoterapiya. Pediatriya (Effective Pharmacotherapy. Pediatrics). 2011; (29): 16-21. (In Russ). |
| [9] | Zakharova I.N, Kuchina A.E. Breast milk microbiota (concept, sources, the role of bacteria for child and mother). Meditsinskiy sovet (Medical Council). 2022; 16(1): 27-35. (In Russ). |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML