-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(1): 374-376
doi:10.5923/j.ajmms.20261601.77
Received: Dec. 29, 2025; Accepted: Jan. 20, 2026; Published: Jan. 28, 2026

Efficiency of Prediction and Early Diagnosis of Preeclampsia
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAtkhamova Sh. R., Kurbanov B. B.
Tashkent State Medical University, Uzbekistan
Correspondence to: Atkhamova Sh. R., Tashkent State Medical University, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

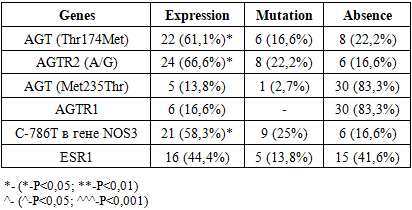
Preeclampsia is a common complication of pregnancy, accompanied by high maternal morbidity and mortality, as well as intrauterine growth retardation of the fetus. The aim of the study was to evaluate the effectiveness of the algorithm proposed by us as a forecast and early diagnosis of preeclampsia in pregnant women. Materials and methods: we examined 36 pregnant women in the second trimester of gestation (20-24 weeks). The study included collecting anamnesis, clinical and laboratory data, and determining allelic genes - AGT (Thr174Met), AGT (Met235Thr), AGTR2 (A / G), AGTR1, C-786T of the NOS3 gene, and ESR1. Results: in most cases, the examined women showed expression of the AGT (Thr174Met), AGTR2 (A / G), C-786T genes in the NOS3 gene, namely 61.1%, 66.6%, 58.3%, respectively. Mutations and the appearance of wild alleles were noted in these genes - 16.6%, 22.2%, and 25%, respectively. The ESR1 gene showed expression in 44.4% of cases, and was detected as mutational variants in 13.8%. Allelic genes AGT (Met235Thr) and AGTR1 did not show significant changes in the examined women. Conclusions: Thus, the obtained data indicate a high independent role of genes AGT (Thr174Met), AGTR2 (A/G) and C-786T in the NOS3 gene in the formation of severe preeclampsia.
Keywords: Pregnancy, Preeclampsia, Endothelium
Cite this paper: Atkhamova Sh. R., Kurbanov B. B., Efficiency of Prediction and Early Diagnosis of Preeclampsia, American Journal of Medicine and Medical Sciences, Vol. 16 No. 1, 2026, pp. 374-376. doi: 10.5923/j.ajmms.20261601.77.
1. Background
- Preeclampsia is a serious pathological condition during pregnancy, with a multisystem nature. It is part of the so-called "Major Obstetric Syndromes," occurring in 3-5% of pregnant women and, according to the WHO (2021), is one of the leading causes of maternal and perinatal mortality. Preeclampsia is a multisystem syndrome, a progressive, unpredictable, and serious disease characterized by vasoconstriction, metabolic disturbances, endothelial dysfunction, activation of the coagulation cascade, and hemostatic disorders. [1,4,14].According to the WHO (2021), preeclampsia ranks among the leading causes of maternal mortality worldwide, directly causing premature birth, uterine bleeding, premature detachment of a normally located placenta, fetoplacental dysfunction, etc. [3,6,7]. The primary clinical manifestation of preeclampsia is hypertensive syndrome, characterized by impaired maternal-placental-fetal circulation. Therefore, Doppler assessment of arterial blood flow in this pregnancy complication is of particular clinical interest. The relevance of this problem is also due to the serious consequences of preeclampsia. Many women who have experienced this condition may subsequently develop chronic kidney disease, endocrine disorders, and hypertension. [10].Kidney damage most often manifests as proteinuria due to the pathognomonic lesion of glomerular endotheliosis and associated loss of podocyte integrity. In severe cases, these lesions can lead to nephrotic proteinuria, acute tubular necrosis, and acute kidney injury [9,11]. Liver injury is characterized by periportal inflammation and hepatocellular injury (manifested by right upper quadrant or epigastric pain and transaminitis), subcapsular hematoma, and, rarely, liver failure or rupture. Jaundice and hypoglycemia are rare and late features that distinguish preeclampsia from acute fatty liver of pregnancy. [12].Hematologic manifestations include relative hemoconcentration (if hemolysis is not present), relative neutrophilia, microvascular thrombosis and hemolysis (manifested by elevated lactate dehydrogenase levels), platelet consumption, and, particularly in placental abruption, disseminated intravascular coagulation. Placental abruption likely results from ischemia-reperfusion injury to the maternal uteroplacental vessels. [5].Objective: To evaluate the effectiveness of our proposed algorithm for predicting and early diagnosis of preeclampsia in pregnant women.
2. Materials and Methods
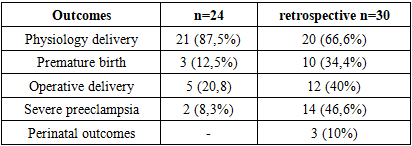
- We studied 36 pregnant women in the second trimester of gestation (20-24 weeks). The study included collecting anamnesis, clinical and laboratory data, and determining allelic genes for AGT (Thr174Met), AGT (Met235Thr), AGTR2 (A/G), AGTR1, C-786T of the NOS3 gene, and ESR1. Expression, mutation, and absence of detection were also measured. The control group retrospectively included 30 pregnant women diagnosed with preeclampsia who had not received preventive measures.Results: When gene expression or the presence of mutational alleles was detected, we classified such women as a risk group and began to carry out preventive measures according to the clinical guidelines of the Ministry of Health of the Republic of Uzbekistan (2016), namely diet (salt restriction), calcium supplements, antiplatelet therapy (acetylsalicylic acid 75 mg), and antihypertensive therapy as indicated.
|
|
3. Conclusions
- Thus, our data demonstrate the significant independent role of the AGT (Thr174Met), AGTR2 (A/G), and C-786T genes in the NOS3 gene in the development of severe preeclampsia. Our proposed algorithm for screening and predicting pregnancy outcomes in women with preeclampsia and at risk for its development is effective and can be implemented in healthcare practice.