-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(1): 371-373
doi:10.5923/j.ajmms.20261601.76
Received: Dec. 18, 2025; Accepted: Jan. 12, 2026; Published: Jan. 28, 2026

Clinical Aspects of Adenomyosis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKurbanov B. B., Mirzamurodova D. A.
Tashkent State Medical University, Uzbekistan
Correspondence to: Kurbanov B. B., Tashkent State Medical University, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Adenomyosis is defined by the presence of the endometrial mucosa in the myometrium. This is probably due to invagination of the basal layer of the endometrium into the myometrium. Objective: to conduct a clinical and anamnestic analysis of women of reproductive age with Adenomyosis. Materials and methods: We analyzed the outpatient records of 93 women of reproductive age diagnosed with Adenomyosis. The examined women were aged 34-43 years. All women were admitted for outpatient treatment to the polyclinic department of the City Interdistrict Perinatal Center No. 6 in Tashkent. The diagnosis of Adenomyosis was established on the basis of complaints, obstetric and gynecological history, as well as ultrasound findings. Results. The main complaints of women admitted for outpatient treatment were pelvic pain, infertility, and vaginal discharge. Pelvic pain was a characteristic symptom, occurring in 83% of women. They reported pelvic pain radiating to the thigh and rectum. Pain during intercourse was reported in 47.3% of cases, which, according to the survey, impaired their libido. Conclusions: Based on the results of our analysis, we can conclude that Adenomyosis has a characteristic aggravated gynecological anamnesis, a pronounced specific clinical picture.
Keywords: Adenomyosis, Uterus, Pain
Cite this paper: Kurbanov B. B., Mirzamurodova D. A., Clinical Aspects of Adenomyosis, American Journal of Medicine and Medical Sciences, Vol. 16 No. 1, 2026, pp. 371-373. doi: 10.5923/j.ajmms.20261601.76.
1. Background
- Adenomyosis is a specific uterine disorder that affects the endometrial glands and stroma, which are irregularly located deep within the myometrium. While previously not considered a distinct entity and attributed to endometriosis, adenomyosis has recently gained prominence. Changes affect not only the uterus and adnexa, but also the entire pelvis. [3,5].The etiology and pathogenetic mechanisms responsible for adenomyosis are poorly understood. Both human and experimental studies support the theory of endometrial intussusception, although de novo adenomyosis may also develop from remnants of extrauterine Müllerian ducts. [4]. The prerequisite for adenomyosis may be either smooth muscle weakness, increased intrauterine pressure, or both. Relatively high estrogen concentrations and impaired immune-mediated growth control in the ectopic endometrium may be necessary for the maintenance of adenomyosis. Smooth muscle hyperplasia and hypertrophy reflect reactive changes secondary to ectopic endometrial proliferation. Further studies are needed to accurately understand the etiology and pathogenesis of adenomyosis. Adenomyosis is a relatively common endomyometrium abnormality, occurring in multiparous women aged 40 to 50 years. [7]. Approximately two-thirds of women experience symptoms such as menorrhagia and dysmenorrhea; uterine leiomyoma is present in 80% of cases of adenomyosis; and adenomyosis is relatively common in women with endometrial adenocarcinoma. Definitive diagnosis is based on findings at hysterectomy, although preoperative diagnostic tests such as magnetic resonance imaging and myometrial biopsy have been attempted. A radical treatment option for women with symptoms is hysterectomy. [5].Adenomyosis frequently affects both the pregnant and non-pregnant uterus, remaining asymptomatic in almost half of cases. Symptoms of adenomyosis, particularly menorrhagia and dysmenorrhea, correlate with the depth of myometrial involvement and, consequently, the patient's age. Adenomyosis most often occurs in women aged 55 to 60 who have given birth. [2,4].Study objective: To conduct a clinical and anamnestic analysis of women of reproductive age with adenomyosis.Study materials and methods: We analyzed the outpatient records of 93 women of reproductive age diagnosed with adenomyosis. The women studied ranged in age from 34 to 43 years. All women were admitted for outpatient treatment to the outpatient department of the Tashkent City Interdistrict Perinatal Center No. 6. The diagnosis of Adenomyosis was established on the basis of complaints, obstetric and gynecological history, as well as ultrasound findings.The study was conducted at the Department of Obstetrics and Gynecology with a Pediatric Gynecology Course at Tashkent State Medical University. We reviewed the outpatient records of women for periods ranging from 6 to 12 months. We examined the course of the disease before and after treatment.
2. Results
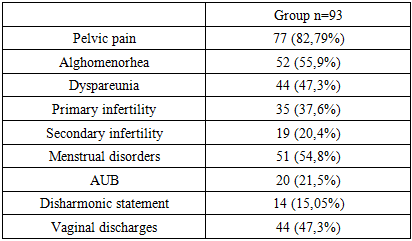
- The main complaints of women admitted for outpatient treatment were pelvic pain, infertility, and vaginal discharge (Table 1). Pelvic pain was a characteristic symptom, occurring in 83% of women. They reported pelvic pain radiating to the thigh and rectum. Pain during intercourse was reported in 47.3% of cases, which, according to the survey, impaired their libido.
|
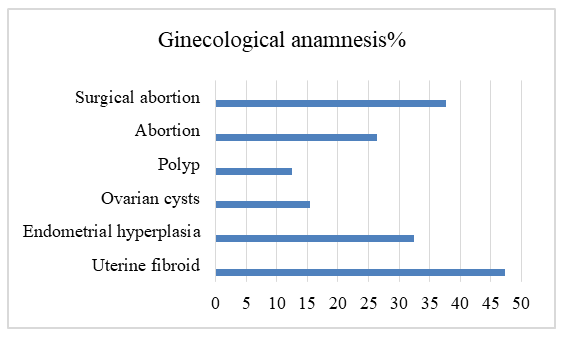 | Figure 1 |
3. Conclusions
- Based on our analysis, we can conclude that adenomyosis is characterized by a complicated gynecological history, a distinct, specific clinical picture, and aggravating lifestyle choices for patients. Ultrasound and histological examination of scrapings are the gold standard for diagnosis, and Dienoges is used for treatment. The search for reliable, informed markers for adenomyosis remains a pressing issue in gynecology.