-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(1): 367-370
doi:10.5923/j.ajmms.20261601.75
Received: Jan. 2, 2026; Accepted: Jan. 23, 2026; Published: Jan. 28, 2026

The Impact of Family Medicine on the Control of Risk Factors for Chronic Heart Failure
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKityan S. A.
Department of Propaedeutic of Internal Medicine, Andijan State Medical Institute, Andijan, Republic of Uzbekistan
Correspondence to: Kityan S. A., Department of Propaedeutic of Internal Medicine, Andijan State Medical Institute, Andijan, Republic of Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This study examines the role of family medicine in the prevention of chronic heart failure at the primary health care level. The analysis identified major cardiovascular risk factors and demonstrated that regular follow-up, risk factor management, and lifestyle modification are associated with improved clinical outcomes. The results emphasize the importance of preventive strategies in family medicine for reducing the burden of chronic heart failure.
Keywords: Chronic heart failure, Prevention, Family medicine, Risk factors
Cite this paper: Kityan S. A., The Impact of Family Medicine on the Control of Risk Factors for Chronic Heart Failure, American Journal of Medicine and Medical Sciences, Vol. 16 No. 1, 2026, pp. 367-370. doi: 10.5923/j.ajmms.20261601.75.
1. Introduction
- Chronic heart failure (CHF) remains one of the most significant challenges in modern medicine, characterized by high prevalence, frequent hospitalizations, and a substantial negative impact on patients’ quality of life [1,4,5]. According to the World Health Organization [19], the incidence of CHF continues to rise, largely due to increasing life expectancy and the growing number of patients with a history of cardiovascular diseases [9,10]. Similar epidemiological trends have been observed in both Russia and Uzbekistan, highlighting the need for active implementation of preventive strategies at the primary health care level [10,15]. The introduction of comprehensive monitoring programs in primary care has been shown to reduce hospitalizations among patients with CHF by approximately 30%; however, mortality associated with CHF remains high, and treatment effectiveness largely depends on the timely identification and control of risk factors. Limited real-world data exist on how long-term family medicine follow-up influences risk factor control in primary care settings in Eastern Europe and Central Asia.Family medicine plays a pivotal role in the prevention of CHF, occupying a central position in primary prevention and long-term patient follow-up [2,3,5,6,9]. Family physicians are able to improve clinical outcomes through early identification of risk factors, lifestyle modification, and the development of individualized preventive strategies. International and national clinical guidelines emphasize that enhancing patient awareness and adherence to treatment is a key component of cardiovascular disease prevention, including CHF [1,11,12,14]. Unlike highly specialized physicians who primarily manage patients with established disease, family physicians have the opportunity to observe patients over extended periods, enabling early detection of predisposing factors and timely implementation of preventive measures.Special attention should be given to CHF prevention in the context of its economic burden on health care systems. Patients with poorly controlled risk factors are hospitalized for CHF-related complications more frequently, leading to a 2.5-fold increase in health care costs and resource utilization [6,9]. A comprehensive approach that includes blood pressure and glycemic control, lifestyle modification (diet, physical activity, and smoking cessation), and early identification of predisposing conditions can substantially reduce the risk of CHF development and improve patient outcomes [3,7,13]. Patient education also plays an essential role in preventive care by fostering a conscious and proactive attitude toward health. Individuals who regularly receive counseling on lifestyle modification demonstrate higher adherence to preventive measures and experience fewer episodes of CHF decompensation. Patients with high adherence to treatment have been shown to have a 40% lower risk of CHF-related complications compared with the control group [12].This article aims to analyze key strategies of family medicine in the prevention of chronic heart failure, focusing on early identification and control of risk factors, the role of family physicians in timely diagnosis and management of patients at risk of CHF, and prospects for the development of preventive programs at the primary care level [2,11,12].
2. Materials and Methods
- The present study is a retrospective observational cohort study based on the analysis of clinical data from 472 patients under long-term follow-up by family physicians in primary health care clinics in Uzbekistan. The study included individuals at increased risk of developing chronic heart failure (CHF), as well as patients with a previously established diagnosis of CHF in a state of clinical compensation.Data were collected over a three-year period, allowing assessment of cardiovascular risk factor dynamics, effectiveness of preventive measures, and patient management characteristics within the framework of family medicine. The cohort included patients aged 40 years and older who had been regularly followed by a family physician for at least two years and had one or more risk factors for CHF, including arterial hypertension, diabetes mellitus, coronary artery disease, and obesity. All participants provided informed consent for the use of their clinical data for research purposes.Exclusion criteria included acute cardiovascular events within six months prior to follow-up, active oncological diseases, and severe comorbidities significantly affecting survival prognosis.Data collection involved analysis of medical records, patient questionnaires, and results of laboratory and instrumental examinations. Cardiovascular risk factors and functional status were assessed according to current clinical guidelines. Blood pressure was measured using standardized office measurements and ambulatory blood pressure monitoring. Other parameters included carbohydrate and lipid metabolism indicators, body mass index and waist circumference, electrocardiography, echocardiography, and frequency of cardiovascular exacerbations and hospitalizations.Statistical Analysis: IBM SPSS Statistics software was used. Quantitative variables were analyzed using the Student’s t-test for independent samples, while categorical variables were compared using the χ² test. Correlation analysis was conducted to assess associations between major clinical and laboratory parameters. Multivariate analyses adjusted for age, sex, and comorbidities were performed to control for potential confounding factors. Differences were considered statistically significant at p < 0.05.
3. Results
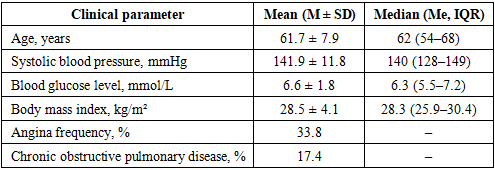
- The study analyzed data from 472 patients who were followed by family physicians over a three-year period. The aim was to identify associations between clinical parameters and adverse outcomes in patients at risk of chronic heart failure (CHF), and to explore the potential benefit of preventive measures implemented in primary care. The demographic and clinical characteristics of the study population are summarized in Table 1.
|
|

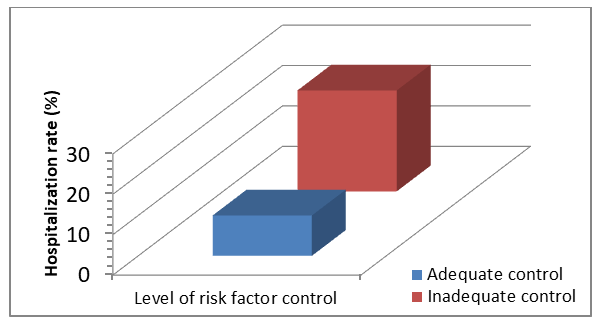 | Figure 1. Frequency of hospitalizations in patients with different levels of risk factor control |
4. Discussion
- The results of the present study are consistent with large epidemiological and clinical studies highlighting the prominent role of arterial hypertension, diabetes mellitus, and obesity in the development of chronic heart failure (CHF) [5,7,9]. The observed associations between blood pressure levels, glycemia, and hospitalization frequency suggest the importance of continuous risk factor monitoring and timely management at the outpatient stage of care [1,3]. Effective control of these modifiable risk factors in primary care may reduce the incidence of acute decompensation episodes requiring hospital admission.Our findings emphasize the potential benefit of early identification and correction of cardiovascular risk factors within the framework of family medicine. This aligns with international reviews and clinical guidelines, which underline that CHF prevention should begin well before the onset of clinical symptoms [1–3,7]. Recent evidence also supports this approach [16–18], highlighting risk-based prevention strategies and the role of structured follow-up, lifestyle interventions, and regular clinical reassessment in primary care settings.Educational and preventive activities carried out by family physicians remain crucial. Increasing patient awareness, promoting adherence to pharmacological therapy, and encouraging lifestyle modifications, including diet and physical activity, may be associated with improved risk factor control and a reduced likelihood of CHF progression. These measures can contribute to earlier detection of clinical deterioration and timely therapeutic adjustments, potentially lowering hospitalization rates. Such strategies are strongly recommended in both international and national guidelines as core components of cardiovascular disease prevention [1,11,12,14].An important aspect of effective CHF prevention is close collaboration between family physicians and cardiologists. While family doctors play a central role in long-term monitoring, risk factor control, and patient education, cardiologists contribute specialized assessment, optimization of complex pharmacotherapy, and management of advanced or high-risk cases. Coordinated care models, including referral pathways and shared decision-making, may enhance continuity of care and improve outcomes for patients at risk of CHF.Limitations of the present study should be acknowledged. First, the retrospective observational design limits the ability to establish causal relationships. Second, the study was conducted within a single-country primary care setting (Uzbekistan), which may affect the generalizability of the findings to other healthcare systems. Third, reliance on medical records and self-reported adherence to lifestyle recommendations may introduce information and reporting bias. Finally, although multivariate analyses adjusted for age, sex, and major comorbidities were performed, residual confounding cannot be completely excluded.Overall, the findings highlight that structured long-term follow-up in family medicine, combined with comprehensive risk factor management, patient education, and collaboration with cardiology specialists, may contribute to improved clinical outcomes and reduced hospitalization rates in patients at risk of CHF. These results provide practical implications for primary care policy, suggesting that strengthening family physician-led preventive programs could be a key strategy in reducing the burden of CHF in Eastern Europe and Central Asia.
5. Conclusions
- The present study demonstrates that family medicine plays a key role in the prevention of chronic heart failure through early identification and correction of modifiable risk factors.Regular patient follow-up, effective control of blood pressure and carbohydrate metabolism, as well as lifestyle modification interventions contribute to a reduction in hospitalization rates and cardiovascular complications.The obtained results confirm the need for further development of preventive programs at the level of primary health care with the active involvement of family physicians and close collaboration with cardiology specialists in the management of patients at risk of chronic heart failure.