-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(1): 362-366
doi:10.5923/j.ajmms.20261601.74
Received: Nov. 22, 2025; Accepted: Dec. 16, 2025; Published: Jan. 28, 2026

Comprehensive Evaluation of Modular Credit System Implementation in Clinical Medical Education: Academic, Digital, and Perceptual Outcomes
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLZafar Zayirovich Aminov
Samarkand State Medical University, Uzbekistan
Correspondence to: Zafar Zayirovich Aminov, Samarkand State Medical University, Uzbekistan.
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

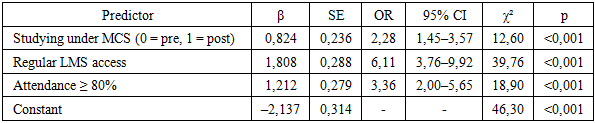
Background. Recent reforms in medical education emphasize personalized learning, digital integration, and competency-based curricula. The modular credit system (MCS), aligned with European standards, is increasingly adopted in medical universities. However, comprehensive assessments of its impact - particularly within clinical disciplines - remain limited. Objective. To evaluate the academic, digital, and perceptual outcomes of MCS implementation in clinical training at a medical university. Methods. A five-year mixed-methods study was conducted at Samarkand State Medical University (2018–2023), involving 320 medical students and 92 faculty members. Two student cohorts were compared (pre- and post-MCS implementation). Data sources included standardized tests, LMS analytics, surveys (Likert scale, AMS-28), e-OSCEs, CRP assessments, portfolios, interviews, and focus groups. Statistical analyses used t-tests, chi-square, Cohen’s d, and logistic regression. Results. MCS implementation led to significant improvements in module completion rates (p<0,001), digital engagement (e.g., sixfold increase in simulation use), and student satisfaction across multiple domains (e.g., curriculum clarity d=0,88, feedback quality d=1,45). Logistic regression showed that LMS usage and in-person attendance strongly predicted academic success (OR=6,11 and 3,36, respectively). Faculty reported improved student discipline but faced challenges related to digital tools and increased workload. Conclusion. MCS yielded measurable academic gains, enhanced digital integration, and improved subjective perceptions of quality and transparency. Successful MCS adoption depends on institutional support, faculty training, and digital infrastructure investment.
Keywords: Modular Credit System, Medical Education Reform, Student Satisfaction, Digital Learning Environment
Cite this paper: Zafar Zayirovich Aminov, Comprehensive Evaluation of Modular Credit System Implementation in Clinical Medical Education: Academic, Digital, and Perceptual Outcomes, American Journal of Medicine and Medical Sciences, Vol. 16 No. 1, 2026, pp. 362-366. doi: 10.5923/j.ajmms.20261601.74.
1. Introduction
- Current trends in medical education reflect a growing demand for flexible, adaptive curricula that align with the accelerating pace of digitalization and rising expectations for physician competency. In response to these challenges, the introduction of a modular credit system (MCS) has emerged as a central component of reform in higher medical education. This approach emphasizes structured competency-based learning, transparent assessment mechanisms, and increased student autonomy [1,6,9].The MCS model, rooted in the principles of the European Credit Transfer and Accumulation System (ECTS), facilitates more efficient organization of the educational process by integrating e-learning platforms, digital tools, and step-by-step knowledge monitoring [4,5,8]. However, the shift toward this system requires substantial changes in teaching practices, enhancement of digital infrastructure, and active adaptation by both faculty and students [2,7].Within medical education, the transition to MCS is particularly relevant given the need to balance intensive theoretical instruction with hands-on clinical training. It also fosters personalized learning pathways and aims to build sustained student motivation [3,10]. Despite regulatory efforts to standardize MCS implementation across universities, empirical data on its effectiveness in specific national contexts remain limited. There is a particular gap in evidence regarding how MCS affects academic performance, digital engagement, and perceived satisfaction among stakeholders [5,6].The aim of this study is to provide a comprehensive evaluation of the impact of the modular credit system on academic outcomes, behavioral indicators, digital engagement, and subjective perceptions of educational quality within clinical disciplines at a medical university.
2. Materials and Methods
- This study was conducted at Samarkand State Medical University over a five-year period from 2018 to 2023. The research design combined elements of a comparative cohort study and a mixed-methods evaluation, allowing for both quantitative and qualitative analysis of the implementation of the modular credit system (MCS) in clinical disciplines.The study population included a total of 320 students from the Faculty of General Medicine. Two cohorts were selected for comparative analysis:Cohort 1 (n=160): students enrolled prior to the implementation of the MCS (2018–2019 academic year),Cohort 2 (n=160): students who studied after full implementation of the MCS (2022–2023 academic year).In addition, 92 faculty members from clinical departments participated in the assessment of pedagogical outcomes, workload, and adaptation to digital tools.A variety of data collection instruments were used:Standardized questionnaires, including the Academic Motivation Scale (AMS-28) and Likert-type satisfaction surveys;Objective Structured Clinical Examinations (e-OSCE) in digital format;Clinical Reasoning Problems (CRP) for assessing critical thinking and clinical decision-making skills;LMS log analytics, tracking engagement metrics such as frequency of access, content completion, and participation in interactive modules;Semi-structured interviews and focus groups with students and faculty;Reflective student portfolios and open-ended narrative responses.For data analysis, both descriptive and inferential statistics were applied. The Student's t-test was used to compare group means, and Cohen’s d was calculated to determine effect sizes. A significance level of p<0,05 was set, with 95% confidence intervals (CI) reported where applicable. Effect size values were interpreted as small (d=0,2), medium (d=0,5), and large (d≥0.8), based on conventional thresholds.Ethical approval for the study was obtained from the university's institutional ethics committee. All participants gave informed consent, and confidentiality was maintained throughout the research process.
3. Results
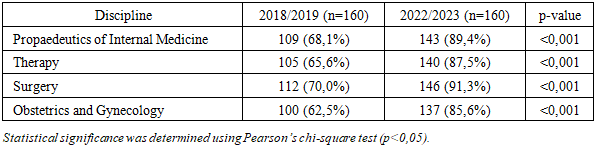
- In addition to quantitative indicators such as academic performance and class attendance, an equally important aspect of evaluating the effectiveness of the modular credit system (MCS) implementation was the assessment of subjective satisfaction among students and faculty, as well as the quality of adaptation to the new educational environment. These data were obtained through surveys, analysis of reflective writings, and expert interviews.The analysis of on-time module completion (Table 1) revealed significant improvements across all major clinical disciplines. For instance, in propaedeutics of internal medicine, 143 students (89,4%) completed the module on time in the 2022/2023 academic year, compared to 109 students (68,1%) in 2018/2019. A similar trend was observed in therapy, surgery, and obstetrics and gynecology, where the proportion of on-time completions increased by more than 20 percentage points in each discipline (p<0,001).
|
|
|
|
|
4. Discussion
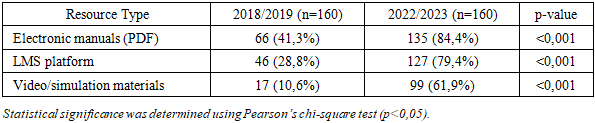
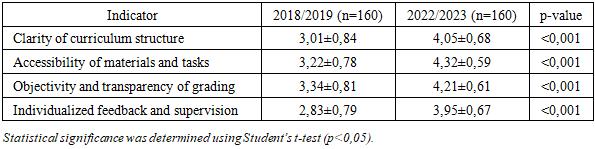
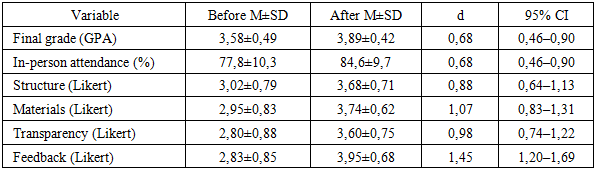
- In addition to quantitative metrics such as academic performance and attendance, a crucial dimension in evaluating the effectiveness of the modular credit system (MCS) implementation was the assessment of subjective satisfaction among students and faculty, as well as the quality of adaptation to the new learning environment. These insights were obtained through surveys, reflective journals, and expert interviews.The findings indicate a positive impact of the MCS on key indicators of educational effectiveness across clinical disciplines. A consistent improvement in academic outcomes was observed: the proportion of students completing modules on time significantly increased across all core subjects - including propaedeutics, internal medicine, surgery, and obstetrics/gynecology. These results are aligned with international studies that highlight the benefits of modular curricula in medical education due to their structured design, periodic assessments, and transparent grading systems [1,6,10].Medium effect sizes in final grades and attendance further confirm the practical significance of the observed changes. Most notably, substantial gains were recorded in subjective dimensions—such as clarity of course structure, transparency in assessment, and personalized feedback. These improvements suggest that the MCS not only enhances measurable academic outcomes but also strengthens students’ trust in the educational system, while fostering intrinsic motivation and learning autonomy [3,6].One of the most significant outcomes was the sharp increase in the use of digital learning tools: a six-fold increase in the use of video materials, a two-fold increase in digital textbooks, and a three-fold increase in LMS engagement. This reflects not only growing digital literacy but also a deeper integration of learning management systems (LMS) into daily teaching practices [2,5,8]. Such patterns echo findings from meta-analyses demonstrating that the incorporation of e-learning resources enhances student engagement and supports academic achievement [5,7,8].Qualitative data from surveys, interviews, and focus groups confirmed broad student acceptance of the reform. Notably, 83% of students reported an improved understanding of course structure, and 76% considered modular assessment to be fair and motivating. However, 21% noted increased workload, especially when balancing theoretical studies with clinical rotations. There were also concerns regarding some faculty’s insufficient digital competence, which was perceived as a barrier to the full implementation of MCS [2,3,9].Faculty responses were more diverse. While many acknowledged improvements in discipline and assessment transparency, only 48% felt fully adapted to the new system. Key challenges included insufficient methodological support, high administrative burden, and the need to adopt new pedagogical roles such as facilitator, mentor, and module curator. These findings underscore the need for institutional support mechanisms - including regular methodological training, access to modular course templates, and technical assistance for LMS use [4,7,9].Particularly noteworthy is the use of effect size analysis, which allowed for standardized comparisons across diverse measurement scales. This approach revealed that subjective components - such as accessibility, clarity, and feedback - were the domains most positively impacted by the reform. These findings emphasize that the success of MCS implementation depends not only on structural changes but also on the quality of pedagogical interaction and the transparency of educational procedures [1,6,10].
5. Conclusions
- In summary, the qualitative findings confirm that the transition to the modular credit system (MCS) was predominantly perceived positively by both students and faculty members. Levels of satisfaction with the learning environment, as well as perceptions of transparency and accessibility of educational information, significantly increased. Digital resources have become an integral component of the educational process. Student adaptation to the new system proved to be relatively rapid and stable, while the facilitative role of instructors and transparent assessment procedures emerged as key factors contributing to the success of the transition. These qualitative insights complement the quantitative results and support the conclusion that the MCS reform has had a comprehensive and positive impact on the academic environment of the university.