-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(1): 325-329
doi:10.5923/j.ajmms.20261601.68
Received: Dec. 30, 2025; Accepted: Jan. 20, 2026; Published: Jan. 26, 2026

Results of Clinical and Functional Examination of Allergic Rhinitis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLJ. A. Djuraev, O. A. Nazarov
Tashkent State Medical University, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

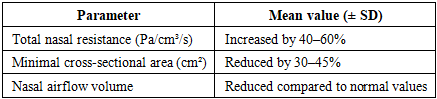
Background: Allergic rhinitis is a highly prevalent IgE-mediated inflammatory disease of the nasal mucosa that significantly impairs nasal breathing and quality of life. Despite its high prevalence, objective functional assessment of nasal airflow remains insufficiently utilized in routine clinical practice. Objective: To evaluate the clinical manifestations and functional characteristics of nasal breathing in patients with allergic rhinitis using integrated clinical examination and objective functional methods. Materials and Methods: A clinical and functional study was conducted in 110 patients with allergic rhinitis treated at the Department of Otorhinolaryngology of the Multidisciplinary Clinic of Tashkent State Medical University between September 2023 and February 2025. All patients underwent comprehensive clinical assessment, anterior rhinoscopy, anterior active rhinomanometry, and acoustic rhinometry. Subjective symptoms were analyzed alongside objective functional parameters of nasal airflow. Results: Nasal obstruction was the predominant symptom, reported by 85–90% of patients, followed by paroxysmal sneezing (70–75%) and watery rhinorrhea (65–70%). Rhinoscopic examination revealed mucosal edema and inferior turbinate hypertrophy in the majority of cases. Functional assessment demonstrated a significant increase in total nasal airway resistance (by 40–60%) and a reduction in the minimal cross-sectional area of the nasal cavity (by 30–45%) compared with reference values. Patients with perennial allergic rhinitis exhibited more persistent symptoms and greater functional impairment than those with seasonal disease. A strong correlation was observed between subjective symptom severity and objective functional indicators of nasal airflow obstruction. Conclusion: Allergic rhinitis is characterized by marked heterogeneity in clinical presentation and functional impairment of nasal breathing. The integration of clinical evaluation with objective functional methods such as rhinomanometry and acoustic rhinometry provides a more accurate assessment of disease severity. This comprehensive diagnostic approach is essential for individualized patient management and optimization of therapeutic strategies.
Keywords: Allergic rhinitis, Nasal obstruction, Rhinomanometry, Acoustic rhinometry, Nasal mucosa, Functional diagnostics
Cite this paper: J. A. Djuraev, O. A. Nazarov, Results of Clinical and Functional Examination of Allergic Rhinitis, American Journal of Medicine and Medical Sciences, Vol. 16 No. 1, 2026, pp. 325-329. doi: 10.5923/j.ajmms.20261601.68.
Article Outline
1. Introduction
- Changes in environmental factors, urbanization, air pollution, industrial waste, climate change, and the intensification of the impact of household and occupational allergens are leading to the widespread occurrence of allergic diseases, in particular allergic rhinitis. At the same time, changes in eating habits, stress factors, genetic predisposition, and increased immune system reactivity also play an important role in the pathogenesis of this disease [1-4]. Allergic rhinitis often begins in childhood and adolescence and persists for years, indicating that the disease has long-term medical and social consequences [5].The relevance of allergic rhinitis is not limited to its prevalence. This disease has a serious negative impact on the quality of life of patients, leading to sleep disturbances, daytime weakness, decreased attention and memory, and reduced productivity in work and studies.Allergic rhinitis is often accompanied by such pathologies as bronchial asthma, chronic rhinosinusitis, nasal polyposis, middle ear diseases, and sleep apnea. According to the ARIA and GINA concepts, the upper and lower respiratory tract are considered a single inflammatory system, and allergic rhinitis is an important risk factor for the development and progression of bronchial asthma [8,9]. Therefore, early detection and correct diagnosis of allergic rhinitis are of great importance not only for ENT practice, but also for pulmonology and general medicine.In ARIA, EPOS, and other international clinical recommendations, the duration of symptoms, severity, and assessment of the functional state of nasal breathing are indicated as the main criteria in the diagnosis of allergic rhinitis. These documents emphasize the need to introduce clinical and functional research methods into daily practice. At the same time, the insufficient use of these methods in developing countries remains a problem.
2. Materials and Methods of Research
- From September 2023 to February 2025, clinical and functional studies were conducted in 110 patients with allergic rhinitis in the Department of Otorhinolaryngology of the Multidisciplinary Clinic of the Tashkent State Medical University. Clinical and functional examination of the nose in allergic rhinitis is important for the correct diagnosis of the disease, determining its severity, and conducting a differential diagnosis. These studies allow us to identify changes in the mucous membrane characteristic of allergic rhinitis, objectively assess the degree of nasal breathing disorders, and monitor the effectiveness of treatment. Clinical and functional studies are complementary methods, the complex application of which significantly increases the accuracy of diagnosis.
3. Results
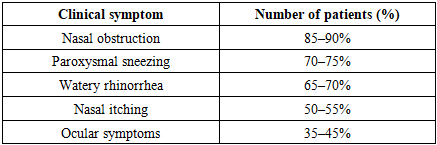
- Clinical studies conducted in patients with allergic rhinitis provide important information regarding the clinical course of the disease, the severity of symptom manifestation, structural changes in the nasal mucosa, and the functional status of nasal breathing. The study included patients of different ages and sexes, in whom clinical symptoms, rhinoscopic findings, and functional parameters were assessed in a comprehensive manner. The obtained results demonstrated the heterogeneous nature of the clinical presentation of allergic rhinitis and highlighted the necessity of an individualized approach to diagnosis and treatment.During the study, the main complaints of the patients were analyzed in detail. Clinical observations revealed that nasal obstruction was the leading symptom in the majority of patients with allergic rhinitis. Most patients reported difficulty in nasal breathing with fluctuations in severity throughout the day, with a marked worsening during nighttime. Paroxysmal sneezing, watery rhinorrhea, and nasal itching were also among the most frequently reported symptoms. In some patients, ocular symptoms such as itching, tearing, and redness were observed, corresponding to the clinical features of allergic rhinoconjunctivitis.According to the results of clinical examination, both the duration and severity of symptoms varied considerably among patients. In individuals with seasonal allergic rhinitis, symptoms predominantly intensified during specific seasons, whereas in patients with perennial allergic rhinitis, symptoms exhibited a more persistent course. This distinction is of significant importance for the clinical classification of the disease and also influenced the results of subsequent functional assessments. The results of the conducted clinical and functional studies provide a comprehensive characterization of the clinical course of allergic rhinitis, the severity and variability of symptoms, morphological changes of the nasal mucosa, and impairments in nasal breathing function. The integrated assessment of subjective complaints, objective clinical findings, and functional parameters allowed for an in-depth evaluation of disease heterogeneity and emphasized the necessity of an individualized approach to diagnosis and management.The study population included patients of different age groups and both sexes, which enabled a broad analysis of clinical manifestations across demographic categories. The mean age of patients was within young and middle adulthood, reflecting the known epidemiological profile of allergic rhinitis. The disease duration varied from newly diagnosed cases to long-standing chronic forms, which allowed for the assessment of symptom progression and functional deterioration over time.Clinical Symptom AssessmentAnalysis of patients’ complaints revealed that nasal obstruction was the most prevalent and clinically significant symptom. The majority of patients reported persistent or intermittent difficulty in nasal breathing, which often intensified during nighttime and early morning hours. Many patients described fluctuations in symptom severity throughout the day, influenced by environmental exposure to allergens, physical activity, and climatic conditions.Paroxysmal sneezing was another frequently reported symptom, often occurring in series and triggered by exposure to allergens such as pollen, house dust, or animal dander. Watery rhinorrhea was commonly observed and was typically associated with increased nasal secretion during periods of allergen exposure. Nasal itching, although less prominent than nasal obstruction and rhinorrhea, was still reported by a substantial proportion of patients and often accompanied sneezing episodes.Ocular symptoms, including itching, tearing, and conjunctival redness, were documented in a considerable number of patients, indicating the presence of allergic rhinoconjunctivitis. These symptoms were more common in patients with seasonal allergic rhinitis and often coincided with peak allergen exposure periods. The presence of ocular symptoms was associated with greater overall disease burden and reduced quality of life.Table 1 summarizes the frequency of major clinical symptoms observed in patients with allergic rhinitis.
|
|
4. Discussion
- The present study provides a comprehensive clinical and functional evaluation of patients with allergic rhinitis and confirms the heterogeneous nature of the disease in terms of symptom severity, mucosal changes, and nasal airflow impairment. The integration of clinical assessment with objective functional methods allowed for a more precise characterization of nasal obstruction and its underlying mechanisms, supporting current international recommendations that emphasize the importance of functional diagnostics in allergic rhinitis.One of the key findings of this study is the predominance of nasal obstruction as the leading symptom among patients with allergic rhinitis. This observation is consistent with data reported in ARIA and EPOS guidelines, which identify nasal obstruction as the most clinically significant symptom affecting quality of life and daily functioning. The high prevalence of nasal obstruction observed in the present study can be explained by persistent mucosal edema of the inferior turbinates, which was frequently detected during rhinoscopic examination. These structural changes contribute directly to increased nasal airway resistance and reduced airflow, as confirmed by rhinomanometric measurements.The study further demonstrated notable differences between seasonal and perennial forms of allergic rhinitis. Patients with seasonal allergic rhinitis exhibited episodic symptom exacerbations related to allergen exposure, whereas those with perennial allergic rhinitis showed more persistent symptoms and more pronounced chronic mucosal changes. This finding aligns with previous studies indicating that continuous exposure to indoor allergens leads to sustained inflammatory activity and progressive mucosal remodeling. The greater functional impairment observed in perennial allergic rhinitis highlights the need for early diagnosis and long-term monitoring in this patient population.Objective functional assessment played a central role in validating subjective complaints. The significant increase in nasal airway resistance and reduction in minimal cross-sectional area measured by rhinomanometry and acoustic rhinometry correlated closely with patient-reported symptom severity. These results support the concept that subjective evaluation alone may be insufficient for accurate assessment of disease severity, particularly in patients who adapt to chronic nasal obstruction. Functional testing provides an objective basis for determining disease severity and treatment efficacy, as emphasized in international consensus documents.The correlation between clinical symptoms and functional parameters observed in this study underscores the diagnostic value of combined clinical and instrumental evaluation. Patients with severe nasal obstruction consistently demonstrated higher resistance values and greater anatomical narrowing, while those with milder symptoms showed relatively preserved nasal airflow. This finding reinforces the role of functional diagnostics not only in confirming the diagnosis but also in guiding individualized treatment strategies and monitoring therapeutic outcomes.From a clinical perspective, the results of this study have important implications for routine practice. The demonstrated variability in clinical presentation and functional impairment indicates that allergic rhinitis should not be approached as a uniform condition. Instead, an individualized diagnostic strategy that incorporates both clinical assessment and objective functional testing is essential, particularly in patients with moderate to severe disease or in cases where symptoms do not correlate with clinical findings.Despite its strengths, the study has certain limitations. The single-center design may limit the generalizability of the results, and the absence of long-term follow-up prevents assessment of disease progression and treatment outcomes over time. Additionally, while functional methods provided objective data, the study did not include biomarker analysis, which could further enhance understanding of inflammatory activity and disease phenotypes. Future research should focus on multicenter studies with longitudinal follow-up and the integration of immunological and molecular markers to refine diagnostic and therapeutic approaches.
5. Conclusions
- This heterogeneity underscores the importance of individualized assessment and management strategies. Functional testing should be considered an essential component of the diagnostic work-up in patients with moderate to severe allergic rhinitis, particularly in cases where subjective complaints do not fully reflect the extent of functional impairment.In summary, the combined analysis of clinical symptoms, rhinoscopic findings, and functional parameters provides a comprehensive understanding of allergic rhinitis and its impact on nasal physiology. The results highlight the need for an integrated diagnostic approach that incorporates both subjective and objective measures to optimize patient care and improve clinical outcomes.
6. Limitations of the Study
- This study has several limitations that should be considered when interpreting the results. First, the research was conducted at a single clinical center, which may limit the generalizability of the findings to broader populations with different demographic, environmental, or healthcare characteristics. Multicenter studies would provide more representative data and strengthen external validity.Second, the study design was observational and cross-sectional, which does not allow assessment of disease progression or long-term changes in clinical and functional parameters. Consequently, the dynamics of nasal airflow impairment over time and the effects of therapeutic interventions could not be evaluated.Third, although objective functional methods such as rhinomanometry and acoustic rhinometry were used, the study did not include immunological or biochemical markers (e.g., serum IgE levels, eosinophil counts, or nasal cytology). The absence of these markers limits the ability to correlate functional impairment with the underlying inflammatory activity and to differentiate between allergic phenotypes.Fourth, the sample size, while sufficient for descriptive and correlation analysis, may not be adequate for detailed subgroup comparisons, particularly between seasonal and perennial forms of allergic rhinitis or across different age groups. Larger cohorts would allow more robust statistical analysis and stratification.Finally, patient-reported symptoms were assessed using clinical interviews rather than standardized quality-of-life questionnaires, which may introduce subjective bias. The inclusion of validated instruments such as disease-specific quality-of-life scales would enhance the precision of symptom evaluation in future studies.Despite these limitations, the study provides valuable clinical and functional insights into allergic rhinitis and supports the use of integrated diagnostic approaches in routine practice.