Mardonov Zhonibek Numonovich, Khamdamov Bakhtiyor Zarifovich, Makhmanazarov Orifjon Mirzonazarovich
Bukhara Medical Institute, Bukhara, Uzbekistan
Correspondence to: Mardonov Zhonibek Numonovich, Bukhara Medical Institute, Bukhara, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The integration of the COLP scale into the LDA allowed us to differentiate the indications for two proprietary surgical methods: baropodometrically guided mini-exostectomy and limited correction of the osseous support of the lesion. Elimination of the pathological support surface resulted in a more than twofold reduction in local peak pressure, a 4.1-fold reduction in the displacement of the support center, and the disappearance of the pathological support axis in 88% of patients.
Keywords:
Hyperkeratosis, Foot deformity, Diabetes mellitus
Cite this paper: Mardonov Zhonibek Numonovich, Khamdamov Bakhtiyor Zarifovich, Makhmanazarov Orifjon Mirzonazarovich, Methods of Surgical Treatment of Hyperkeratosis and Early Foot Deformities in Patients with Diabetes Mellitus, American Journal of Medicine and Medical Sciences, Vol. 16 No. 1, 2026, pp. 312-317. doi: 10.5923/j.ajmms.20261601.66.
1. Introduction
Issues related to the early detection and treatment of hyperkeratosis and overload foot deformities in diabetes mellitus have been the subject of repeated research in both clinical endocrinology and orthopedic surgery in recent years. Despite the diversity of approaches, a significant portion of the studies reflects primarily attempts to control the consequences of pathological loading rather than its underlying cause. As demonstrated in a recent literature review, most available studies focus on eliminating hyperkeratosis, treating preulcerative lesions, and preventing ulcerative defects, while issues of correcting structural support and biomechanical stability of the forefoot remain fragmented [1,3,5].Removing hyperkeratosis and using relieving insoles and therapeutic footwear provide only temporary load reduction, as they do not address the structural cause of the overload. Researchers have similarly concluded that even with regular podiatric treatment, the recurrence of hyperkeratosis in the same location is considered a normal course of the disease, as the underlying bone support remains unchanged. As a result, clinical interventions provide short-term results and do not prevent the mechanical cycle of repeated injuries, which explains the consistently high recurrence rate [2,4,6].Several studies have attempted to use baropodometry methods to stratify risk and identify areas of overload. Quantitative assessment of plantar pressure does allow for the detection of persistent localized load peaks, but in most clinical studies, the resulting values were interpreted only as an auxiliary diagnostic guide. A similar position is expressed by some studies, which emphasize that baropodometry is rarely integrated into surgical selection algorithms and is practically never used to determine indications for interventions on bone support. As a result, the detection of a pronounced pressure peak records the fact of the violation itself, but does not form the basis for systemic decision-making on the correction of pathological support [7,9].Approaches based on the analysis of clinical observations also failed to identify transitional states, such as a latent preulcer cavity, recurrent hyperkeratosis, or initial signs of osteolysis, and to consider them as interrelated stages of a single pathogenetic process [8,10]. Literature reviews emphasize that even with the availability of instrumental data, attempts to integrate them into tactical decisions remained fragmented, and risk criteria were formed primarily empirically, without reliance on multifactorial models.At the surgical level, the level of study also remains insufficient. Attempts have been made to perform local bone corrections; however, these interventions are extremely limited in the literature and have been interpreted as modifications of resections for the treatment of established ulcers or neuroosteoarthropathy.Thus, the degree of study of the problem is characterized by fragmentary approaches, the absence of integrative diagnostic criteria and insufficient development of minor bone-unloading operations as a method of early surgical correction, which confirms the need for a comprehensive study aimed at constructing a quantitative model of overload and creating optimized surgical tactics.The aim of the study: to develop methods for surgical treatment of hyperkeratosis and early foot deformities in patients with diabetes mellitus.
2. Materials and Methods
To objectively assess the condition of the foot and develop a tool for the formation of a substantiated surgical approach, a retrospective analysis revealed the need to divide patients into subgroups depending on the presence or absence of NPP. This approach allowed us to compare the clinical, baropodometric, and other characteristics of the lesion in two fundamentally different clinical situations. The first subgroup included 38 patients (52.8%) with hyperkeratosis without signs of NPP and probability to the bone; the inclusion criteria were the absence of a soft tissue defect, the absence of severe inflammation, and the absence of subepithelial cavities according to ultrasound data. The second subgroup included 34 patients (47.2%) with NPP, confirmed by a combination of clinical signs (the presence of a defect, maceration, infiltration), a positive probing test, local hyperthermia, and signs of overload involvement of bone structures. This distribution of patients made it possible to form a balanced basis for further analysis and identification of criteria necessary for an objective assessment of the pathological support and the selection of a justified surgical tactic.A comprehensive analysis of clinical, laboratory, and instrumental diagnostic data revealed that traditional verification of hyperkeratosis and associated foot lesions captured only the superficial manifestations of the process, while key pathogenesis elements remained unnoticed. Clinical signs identified complaints, inflammation, and fungal infection, but did not reflect the degree of structural failure of the forefoot. Laboratory parameters demonstrated a progressive inflammatory background and more frequent decompensation of diabetes in patients with NUP, but these changes became noticeable only at an advanced stage of the lesion. Instrumental diagnostics revealed significant bone changes and characteristic signs of localized overload even in patients with little or no clinical deformity. This discrepancy between different assessment levels indicates the lack of a unified system for analyzing the lesion and emphasizes that the traditional approach did not adequately stratify patients or create the conditions for choosing the correct surgical approach, which became the primary prerequisite for the transition to the development of a new diagnostic and treatment model.
3. Results and Discussion
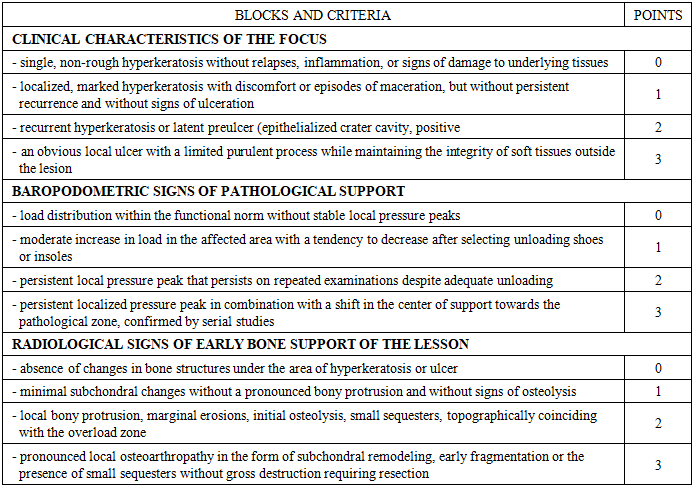
The results of the multivariate logistic analysis allowed us to quantify the contribution of each parameter to the need for local bone-unloading correction and use these data to construct a comprehensive assessment scale for local overload and bone support of the "COLP" lesion. The scale is organized into three sections, reflecting clinical manifestations, baropodometric characteristics of foot support, and radiographic signs of early bone structure and configuration changes. Each block includes four levels of symptom severity, assigned a score from 0 to 3. This approach ensures a sequential transition from minimal to severe changes, covering the full spectrum of conditions identified in the control group (Table 1). The first block captures the clinical features of the lesion and begins with mild hyperkeratosis, which is assigned a score of 0 as a condition without signs of structural instability. Increasing hyperkeratosis severity, the appearance of discomfort, and episodes of maceration correspond to a score of 1. The most important category within the clinical block is the combination of recurrent hyperkeratosis and an epithelialized subepithelial cavity, reflecting the presence of a latent preulcer; this condition is assigned a score of 2.Table 1. COLP diagnostic scale for hyperkeratosis of the foot in patients with diabetes
 |
| |
|
The highest severity (3 points) corresponds to a formed ulcer with a localized purulent process in the absence of systemic manifestations. The depth of the defect according to the Wagner classification is recorded separately and is not included in the scoring. This gradation allows for the consideration of three key stages of damage (hyperkeratosis, preulcer, and ulcer), each with its own prognostic value.The second block reflects baropodometric signs of pathological support. A score of 0 points is assigned for normal load distribution. A moderate increase in pressure, compensated for by orthopedic devices, is assigned 1 point. A persistent localized peak, persisting during repeated examinations, corresponds to 2 points, indicating stable biomechanical overload. The most pronounced impairment, in the form of a persistent peak in pressure, accompanied by a shift in the center of support toward the pathological zone, is assigned 3 points. This sequence replicates the gradient of the contribution of overload factors revealed by statistical analysis and ensures an accurate quantitative reflection of biomechanical impairments.The third block describes the radiographic signs of early bone support of the lesion and begins with a score of 0, indicating no changes in the bone structures beneath the lesion. Minimal subchondral changes are recorded as a score of 1. A score of 2 corresponds to a localized bony prominence, erosions, and initial signs of osteolysis, reflecting the formation of a primary support zone beneath the soft tissue lesion. The maximum severity of the disorder is assessed at 3 points and includes signs of localized osteoarthropathy, subchondral remodeling, and the presence of small sequesters that do not require extensive resection. This structure allows for the consideration of both early and advanced signs of overloaded skeletal remodeling, which are key factors in determining the surgical approach.Assigning a specific score to each feature allows for the formation of a summary assessment of the lesion's condition, enabling the scale to be integrated into a digital environment. The scoring system was adapted to the machine learning module, in which the values of each level were included in the model as independent predictors. The algorithm analyzed combinations of characteristics in three blocks and generated a probabilistic assessment of the severity of pathological support. In the absence of baropodometry or radiographic data, it used clinical and biomechanical patterns established during training. This enabled partial substitution of missing data and significantly reduced the diagnostic burden during initial consultations.The developed scale served as the basis for subsequent evaluation of its diagnostic effectiveness and comparison with traditional examination methods. This will allow us to determine its value as a tool for choosing surgical treatment strategies and move on to an analysis comparing various diagnostic methods.The development of the "KOLP" scale for a comprehensive assessment of localized overload and bone support in a lesion allowed for a quantitative characterization of the severity of pathological support and the creation of a numerical indicator reflecting a combination of clinical changes, biomechanical abnormalities, and early bone remodeling. The total score on the "KOLP" scale has proven to be a convenient tool for classifying patients into three groups, differing in the risk of lesion progression and the likelihood of the need for localized bone-unloading correction. This classification allows for a transition from a fragmented assessment of the lesion to a decision-making structure, where each score range defines its own LDA trajectory.Patients with a score of ≤ 2 points are classified as requiring conservative measures at the soft tissue level. This group is dominated by conditions in which impairments are limited to the superficial layers without persistent biomechanical overload and without evidence of structural support from bony elements. The combination of minimal clinical activity and the absence of persistent pressure peaks allows these patients to be managed under surgical supervision, limited to soft-tissue intervention, orthopedic unloading, and dynamic observation.The 3-5 point range forms a borderline risk zone, where lesions are more often characterized by an epithelialized subhypertensive cavity, initial bone remodeling, or a localized pressure peak that persists during repeated examinations. In this group, the precise choice of strategy requires repeated instrumental assessment and allows for variability: with favorable dynamics, a de-escalation to conservative methods is possible, while with increasing impairment, a transition to local bone correction becomes necessary.A score of ≥ 6 points defines a zone with a high probability of performing local bone unloading surgery. In these patients, persistent overload is combined with significant bone support of the lesion, creating conditions for relapse, the formation of new defects, and progressive destruction. In this group, the optimal strategy involves performing one of the developed minor bone surgeries aimed at eliminating the structural source of pressure and restoring balanced support.The transition to a LDA for choosing a surgical strategy requires combining the obtained scoring system with a sequence of clinical decisions that form a tree of actions, in which each zone defines its own branch, and the dynamics of the lesion's condition determines the possibility of escalation or de-escalation. The construction of such a LDA is the next stage of our development.LDA begins with an assessment of blood flow, as this stage defines the applicability boundary for all subsequent tactics. Ultrasound Doppler imaging and determination of the ABI allow us to identify patients with critical ischemia, who require a different sequence of actions. Such situations place the patient outside the developed scheme, since eliminating local congestion is of no benefit in the presence of severe angiopathy and ischemic SDS. If blood flow is preserved or compensated, the patient is transferred to the next stage of LDA, which is based on the total scores on the "COLP" scale. Unlike traditional approaches, the choice of further actions is determined not by individual clinical signs, but by an integrated assessment of the lesion's condition. The low total score branch, including values ≤ 2 points, corresponds to a condition in which there is no significant overload and no signs of bony support for the defect. Treatment at this level is limited to soft tissue interventions. Examination and treatment of hyperkeratosis are supplemented by orthopedic unloading and the selection of footwear that can adjust pressure distribution. Follow-up examinations are aimed at assessing the load dynamics and preventing the condition from reaching the borderline zone. In the absence of signs of deterioration, the patient remains in this branch of the LDA. The development of an epithelialized cavity or the emergence of a persistent peak in podoscopic pressure during a repeat assessment leads to an escalation of the treatment strategy and a recalculation of the total score. The borderline zone includes patients with a score of 3-5 points, and early signs of structural instability are often detected in this group. Repeat baropodometry and radiographic examination are necessary to clarify the degree of involvement of bony support and the nature of the overload.At this level, the pre-ulcer or minor defect is debrided, hyperkeratosis is eliminated, orthopedic correction is enhanced, and the area of maximum pressure is relieved. The patient is monitored dynamically, allowing for an assessment of the tendency toward decreased load or, conversely, stabilization at the level requiring intervention. If the severity of the abnormalities decreases and the total score drops to <3, a return to conservative management is possible. If the load increases, new radiographic changes appear, or the total score enters the high-risk range, the patient is transferred to the next branch of the LDA.The high-risk zone is formed when the total score is ≥6 points. These patients are characterized by persistent overload and the presence of significant bone support of the lesion, which creates the conditions for recurrent ulcers and chronicity. In this branch, the LDA involves performing local bone-relieving surgery. The choice of intervention is determined by the nature of the bone deformity and the biomechanical load pattern. The postoperative phase includes soft tissue debridement, orthopedic unloading, and mandatory load distribution monitoring.Repeat baropodometric and radiographic assessments help determine whether the support pattern has been achieved or whether an adjustment to the intervention is required. If the postoperative total score drops to <3, the patient is transferred to the low-risk zone, which corresponds to de-escalation of the strategy. If persistent signs of overload persist, additional correction is performed or alternative surgical solutions are considered.The LDA structure allows for controlled patient movement between tactical zones. Escalation is used in situations where overload or bone changes increase and the likelihood of an unfavorable outcome increases. De-escalation becomes possible with sustained positive dynamics after the intervention or conservative treatment. This system provides a clear sequence of actions, is based on the results of multivariate analysis, and forms the basis for the application of surgical techniques appropriate to the level of structural instability.The development of a surgical approach based on LDA has identified two standard surgical options aimed at eliminating the bony support of the pathological zone and reducing localized overload. These procedures do not duplicate standard exostectomies and minor resections, but are modified versions based on baropodometry data and early structural changes in the affected area. This approach allows for interventions to be performed in accordance with the actual biomechanics of the patient's foot, increasing the accuracy of correction and reducing the likelihood of hyperkeratosis recurrence or the formation of a new risk zone.The first intervention option was a baropodometry-guided mini-exostectomy, used when a bony protrusion or localized metatarsal head remodeling is detected, leading to persistent increased load. The surgery is based on preliminary determination of the direction and magnitude of peak pressure, allowing for targeted removal of the bony support point. Unlike the standard "cutting" of the protrusion, which is performed without quantitative reference points, the modified technique involves creating a flat support surface with an adjusted resection angle in accordance with the direction of the pathological load. This strategy allows for pressure redistribution to adjacent structures without creating a new overload zone. After protrusion removal, the bone surface is reshaped so that it does not create a localized pressure peak within the physiological support axis. A soft tissue debridement stage complements the procedure, but the primary effect is achieved by correcting the bone relief, which eliminates the key pathogenetic link.The surgical technique is a baropodometrically guided mini-exostectomy. The incision is made in the projection of the pathologically overloaded metatarsal head, as determined by baropodometry data. The incision is directed longitudinally or slightly arched along the axis of the metatarsal bone, 1.5-2.0 cm long, allowing access to the bony protrusion with minimal trauma. The skin is incised with a scalpel, and then, under sharp dissection, the subcutaneous tissue is divided to the level of the fascia. Bleeding vessels are coagulated with a bipolar electrocoagulator to prevent hematoma formation. The fascia is sharply incised longitudinally, exposing the metatarsal head. The bony prominence is exposed under visual control using soft tissue retractors, avoiding excessive tension on the joint capsule. After exposure of the pathological area, it is assessed against the direction of peak pressure determined during preoperative baropodometry. Resection is performed with an oscillating saw or mini-chisel, strictly in the plane of the pathological load, which eliminates the point of overload without disrupting the anatomical axis of the metatarsal bone. The resection angle is adjusted according to the pressure vector, avoiding the formation of a "step" or localized protrusion on the opposite side. The resection surface is ground with a burr or rasp to create a smooth support surface to prevent the recurrence of peak load zones. During the bone surface modeling stage, attention is paid to creating a single, smooth support line without abrupt transitions. If necessary, minimal reshaping of adjacent areas of the metatarsal head is performed if they could potentially become new pressure peaks. After completing the bone stage, the wound is irrigated with isotonic solution, removing bone dust and osteotomy fragments. Soft tissue debridement involves excision of fibrously altered areas of the capsule and release of tendon fibers under constant compression, which improves joint mobility and reduces the risk of cicatricial contracture.After hemostasis is verified, the fascia is closed with absorbable material using a continuous suture. The subcutaneous tissue is adjusted with interrupted sutures. The skin is sutured with 5/0 nylon or polypropylene, ensuring atraumatic adaptation of the edges. A sterile, aseptic dressing with gentle compression is applied to the wound, preventing excessive pressure on the osteotomy site. Foot immobilization is performed, if necessary, with a custom-made unloading insole or minimal immobilization for 5-7 days, followed by early functional loading along the transferred axis.The second intervention option was limited correction of the bone support of the lesion in the presence of early signs of osteolysis, erosion, or subchondral remodeling. This procedure is used when structural changes are detected that are at a stage preceding severe destruction. Correction is performed within the zone determined by instrumental examinations, eliminating excess load-bearing without affecting healthy bone. During the procedure, small fragments involved in the formation of the pathological support surface are removed and the relief is remodeled to match the load distribution characteristic of a healthy foot. This approach reduces the risk of progression and ensures more precise restoration of the support trajectory. The advantage of the surgery is minimal trauma and preservation of structures that can provide stability to the forefoot after restoration.The surgical technique involves limited correction of the bone support of the lesion. The surgical approach is planned based on the location of the pathological load, determined by baropodometry. The incision direction is chosen along the axis of the corresponding metatarsal bone, usually longitudinal, with a length of 1.5-2 cm. After layer-by-layer dissection of the skin and subcutaneous tissue, careful hemostasis is performed with bipolar coagulation, which prevents the formation of a dense hematoma and subsequent fibrous deformity. The fascia is opened with a longitudinal dissection, then soft retractors are used to spread the tissues, exposing the metatarsal head. At this stage, anatomical landmarks are compared with baropodometry data, determining the precise zone of maximum pressure and the area that forms the load "peak." After visualizing the bony protrusion or localized remodeling of the support surface, limited correction is performed. Resection is performed with an oscillating saw or miniature chisel in the direction of the pathological force vector, eliminating misaligned resection. The cutting angle is individually selected, based on preoperative data on the direction of the pressure center shift. The primary goal is to restore the smooth contour of the bone support without creating a new point of overload on the opposite side. After removal of the protrusion, the bone surface is carefully modeled with a rasp or small cutters, achieving a flat, smooth support surface that does not create localized pressure zones under physiological loading. If necessary, minimal correction of adjacent areas is performed if they could potentially become secondary peak points. Additionally, the capsule and adjacent soft tissues undergo sanitizing treatment, i.e., fibrously altered areas are excised, tendon structures are freed from compressive scar tissue, which reduces the risk of limited mobility and promotes uniform load distribution in the postoperative period.After completing the modeling, the wound is irrigated with an isotonic solution and hemostasis is monitored. The fascia is closed with absorbable material, and the subcutaneous layer is adapted with interrupted 5/0 monofilament sutures. An aseptic dressing and gentle compression are applied, avoiding direct pressure on the area of bone correction. In some cases, an unloading insole or special shoes are used with proximal support for 5-7 days, after which the patient is transferred to graduated functional loading.The combined use of these two interventions allows for the elimination of both pronounced bony protrusions and hidden bony support in the early stages of the lesion. Surgeries are performed according to a biomechanical load model generated by baropodometry data and confirmed by radiographic assessment of the bone architecture.In all cases, postoperative management includes the use of orthopedic unloading, monitoring of pressure distribution, and re-evaluation of the support contour. This approach allows for timely adjustments to treatment strategies and prevents the recurrence of abnormal loading patterns, reducing the risk of relapse and improving functional treatment outcomes.The use of the proposed LDA has enabled the development of a consistent decision-making system based on a quantitative assessment of the degree of local overload and early signs of bony support of the lesion. This has made it possible to limit surgical interventions to those deemed pathogenetically justified. This approach allows for controlled escalation and de-escalation depending on the dynamics of the foot's condition, while the implementation of modified minor surgeries allows for the correction of structural abnormalities at key stages of progression. The completeness of the LDA and its connection with objective diagnostic methods create the conditions for testing its clinical applicability. The next step is to conduct a comparative assessment of the effectiveness of the proposed approach versus traditional treatment methods, which will determine its contribution to improved outcomes and confirm the feasibility of integrating the LDA into clinical practice.
4. Conclusions
1. Multivariate logistic analysis enabled us to identify independent predictors of local unloading surgery, with sustained peak pressure, center of support displacement, and early bone changes having the greatest impact. Based on the obtained coefficients, a three-component "COLP" scale was constructed, incorporating clinical, biomechanical, and radiographic features.2. The comprehensive model demonstrated high sensitivity (84.6%) and specificity (88.2%), enabling the scale to be used as a tool for objective risk stratification and the formation of structured LDA-based tactical decisions.
References
| [1] | Apsamatov N.K., Khamidzhan Uulu A., Maratov N.M. and others. Diagnosis and treatment of SDS at the present stage // Bulletin of Science and Practice. - 2025. - T. 11, No. 6. - P. 196-208. |
| [2] | Bregovsky V.B., Demina A.G., Karpova I.A. et al. Relapses of foot ulcers in patients with diabetes in outpatient practice // Bulletin of surgery named after. I.I. Grekova. - 2022. - T. 181, No. 2. - P. 49-56. |
| [3] | Egiazaryan K.A., Miroshnikova E.A., Zhavoronkov E.A. and others. Analysis of the results of surgical treatment of complex forefoot deformities in older patients // Politravma. - 2021. - No. 3. - P. 46-53. |
| [4] | Makhmudova L.Sh., Muratova S.N. Podological care for patients with diabetic foot syndrome // Student science and medicine of the 21st century: traditions, innovations and priorities. SMART: XVI All-Russian (90th final) student scientific conference of the Student Scientific Society with international participation: materials, Samara, April 13-14, 2022. - Samara: OOO SamLuxPrint, 2022. - P. 119-120. |
| [5] | Okhunov A.O., Kasimov U.K., Atakov S.S. Results of using different types of open osteotomies of the fifth metatarsal bone in Taylor's deformity // Young Specialist. - 2023. - No. 5(14). - P. 3-13. |
| [6] | Tsed A.N., Ilyushchenko K.G., Dulaev A.K. et al. Results of using different types of open osteotomies of the fifth metatarsal bone in Taylor's deformity // Bulletin of Surgery named after I.I. Grekov. - 2025. - Vol. 184, No. 2. - P. 43-51. |
| [7] | Albulescu R., Dima S.O., Florea I.R. et al. COVID-19 and diabetes mellitus: unraveling the hypotheses that worsen the prognosis (review) // Exp Ther Med. - 2020. - Vol. 20, No. 6. - P. 194. |
| [8] | Alsabek M.B., Abdul Aziz A.R. Diabetic foot ulcer, the effect of resource-poor environments on healing time and direct cost: a cohort study during Syrian crisis // Int Wound J. - 2022. - Vol. 19, No. 3. - P. 531-537. |
| [9] | D'Souza R.S., Barman R., Joseph A., Abd-Elsayed A. Evidence-based treatment of painful diabetic neuropathy: a systematic review // Curr Pain Headache Rep. - 2022. - Vol. 26, No. 8. - P. 583-594. |
| [10] | Liu Y., Zhang H. Recurrence patterns of diabetic foot ulcers and inadequacy of traditional clinical risk models: a systematic review of Chinese cohorts // Front Endocrinol (Lausanne). - 2024. - Vol. 15. - P. 1387221. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML