-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(1): 283-287
doi:10.5923/j.ajmms.20261601.62
Received: Dec. 28, 2025; Accepted: Jan. 17, 2026; Published: Jan. 26, 2026

Pathomorphology of Mesenteric Lymph Nodes in Infants Who Died from Peritonitis in the Neonatal Period
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLEshbaev Erkin Abdukhalimovich1, Boltaboev Tulkinboy Tursunalievich2
1DSc, Professor, Department of Pathological Anatomy, Tashkent State Medical University, Tashkent, Uzbekistan
2Independent Researcher, Fergana Medical Institute of Public Health, Fergana, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Peritonitis in infants in the neonatal period, mainly primary hematogenous, lymphogenous foci, necrotic enterocolitis, is a process that occurs in the perforation of the intestines, and as a result of sepsis, septicopyemia, purulent inflammation of all layers of the peritoneum, in addition to massive atrophic, sclerotic changes in the regional lymph nodes, acute insufficiency of all morphofunctional layers, leading to T and B cell collapse, delymphatization in the lymph node and lymph node reticulocytosis. It was found that in the subcapsular and medullary layers of the lymph node, coarsely dispersed proteinaceous deposits consisting of various damaged tissue and cell components were accumulated.
Keywords: Lymph node, Peritonitis, Lymphoid follicle, Immunodeficiency, Infant
Cite this paper: Eshbaev Erkin Abdukhalimovich, Boltaboev Tulkinboy Tursunalievich, Pathomorphology of Mesenteric Lymph Nodes in Infants Who Died from Peritonitis in the Neonatal Period, American Journal of Medicine and Medical Sciences, Vol. 16 No. 1, 2026, pp. 283-287. doi: 10.5923/j.ajmms.20261601.62.
Article Outline
1. Introduction
- Perinatal and neonatal mortality associated with generalized inflammatory processes, including peritonitis, continues to occupy a significant place in the structure of causes of death in newborns. Neonatal peritonitis is characterized by a fulminant course, a high incidence of septic complications, and an unfavorable prognosis, especially in premature infants and those with morphofunctional immaturity [1,2,11]. In the world today, the lethality of purulent peritonitis is very high, reaching 20-60%. When this disease occurs, it is accompanied by the development of rapidly developing endogenous intoxication and multi-organ failure. In the USA and Europe, the incidence rate is 10-15 per 100 thousand, while in Turkey and Korea it is 12-17 per 100 thousand [3,4,6]. In the Russian Federation and the CIS countries, it is 15-20 per 100 thousand, while in Central Asian countries, Azerbaijan, and Armenia this figure is 50-71 per 100, with a lethality rate of 60-85% [3,4,5].In our country, on average, 700-1300 infants under the age of 1 die from various types of peritonitis per year. In peritonitis, the main organs actively involved in the drainage of the abdominal cavity are only the regional lymph nodes, and at 1-3 months of age, this drainage is dominated by the occurrence of physiological paralysis and slow blood circulation, while at 3-6 months, the weakening of intestinal peristalsis and drainage in the regional lymph nodes, insufficiency of the barrier function, lead to the stagnation of local infection in the intestinal lymph nodes and the development of lymphostasis [7,8]. This requires the development of specific recommendations, taking into account the specific morphofunctional aspects of each period [9,10,12]. The insufficient development of morphological criteria for mesenteric lymph node involvement complicates an objective forensic and clinicopathological assessment of the causes of death, the degree of generalization of the inflammatory process, and the severity of the immune response in infants who died during the neonatal period. In addition, the lack of systematized pathomorphological data limits the possibilities for correlating clinical, laboratory, and autopsy findings. Objective Study and improvement of morphological, morphometric, immunohistochemical aspects of regional lymph nodes in peritonitis developed in infants under one year of age.
2. Materials and Methods
- A total of 71 patients, including 12 control group and deceased children, who were brought to the Republican Center for Pathological Anatomy in 2018-2023 were used as material. The samples were stained with hematoxylin and eosin and studied.
3. Results of the Study and Discussion
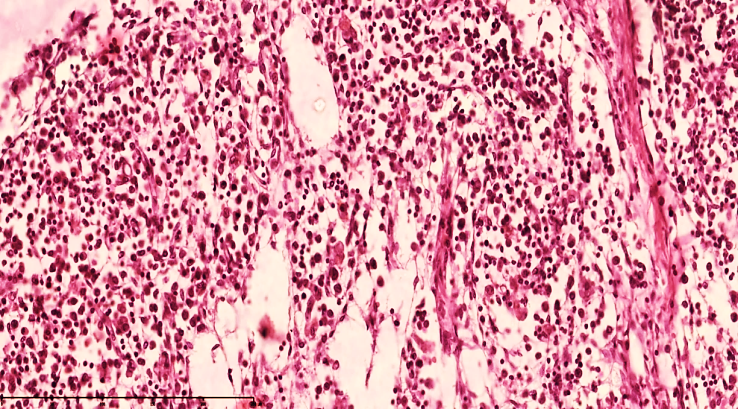
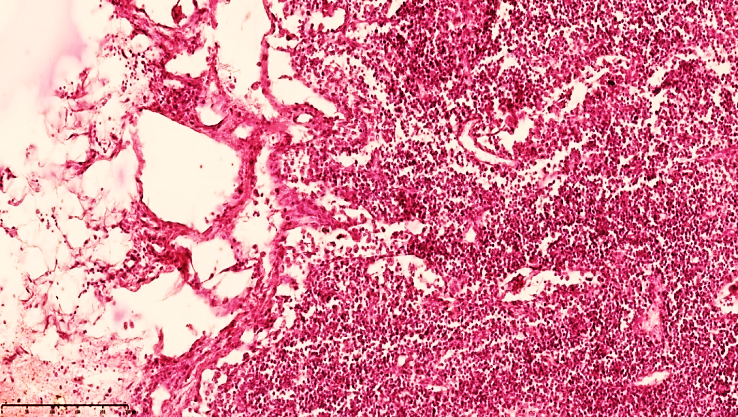
- Microscopic examination of regional lymph nodes in infants who died of peritonitis at 28 days of age revealed that the immature medullary and medullary layers were not fully formed, and changes that occurred as a result of severe large-scale purulent and non-purulent inflammation, such as necrotic enterocolitis, before the development of peritonitis led to changes in the lymphatic drainage system in the form of blockage or paralysis.This, in turn, was manifested by a sharp tightening of the capsule in the mesenteric lymph nodes of 28-day-old infants, a sharp expansion of the subcapsular spaces, which were significantly enlarged. In particular, in the development of peritonitis, a sharp decrease in the function of lymphatic drainage mainly leads to the accumulation of exudate fluid in the abdominal cavity. Hyperproduction of mesothelial cells and the formation of multifocal desquamation foci, many erosive foci were also detected in the visceral sheets.In the mesenteric lymphatic vessels, a sharp slowdown in the drainage function of lymphostasis is observed, which is explained by the expansion of the vessels and the increase in size of the fluid accumulated due to plasmarrhagia in the regional lymph nodes. As a result, the capsules of the lymph nodes are stretched, the subcapsular spaces expand, and lymphostasis develops. Eosinophilic inclusions of varying degrees of light and dark staining in the cortex and medulla of the lymph node: cellular components, various tissue parts with destructive changes were detected. The lymph nodes have a swollen appearance, the capsule is tense, and the subcapsular spaces are filled with lymphatic fluid (see Figure 1). Secondary lymphoid follicles are not detected, the germinal center is quiet, the location of lymphocytes in the cortical and paracortical areas of the active areas of the lymph nodes is reduced compared to normal, and in the active areas of the cortex, foci of lymphocytes migrating towards the postcapillary venules are detected. In the direction of the cerebral bands of the medulla, it is determined that a swelling appearance in the areas of the lymphatic gate and a variable mixture of lymphocytes and other types of cells (macrophages, dendritic cells, interdigitating cells, fibroblasts, histiocytes, reticulocytes, etc.) are relatively preserved in the areas of the reticulum and trabeculae of the brain bands.
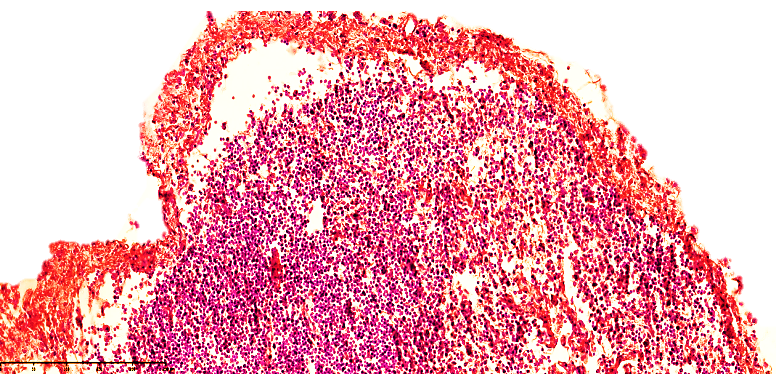 | Figure 1. Mesenteric lymph node of a 28-day-old infant with peritonitis. Treated for 10 days. The lymph node capsule is of variable width, the subcapsular space is dilated, and lymphoid follicles are not identified. Small vessels are fully visible. Stained with GE. Size 10x10 |
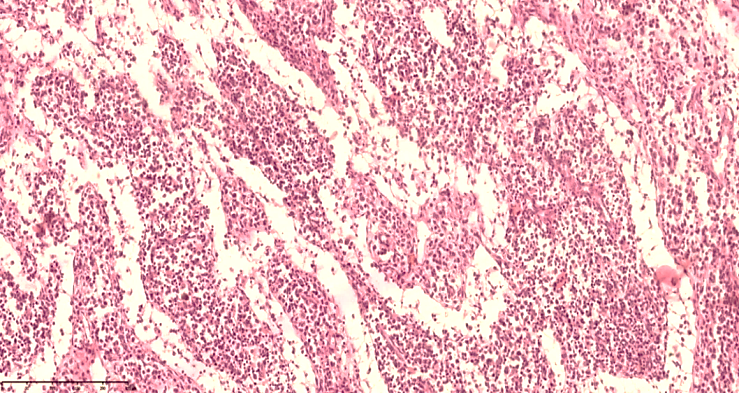
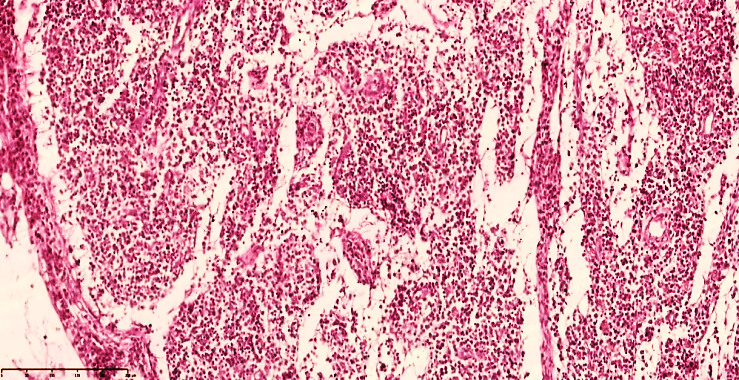 | Figure 2. Mesenteric lymph node of a 28-day-old infant with peritonitis. The capsule is thickened, the subcapsular space is markedly enlarged, the peritrabecular areas are bare, formed in the form of a cavity, and the lymphoid follicles do not have a clear border. Staining G.E. Size 10x10 |
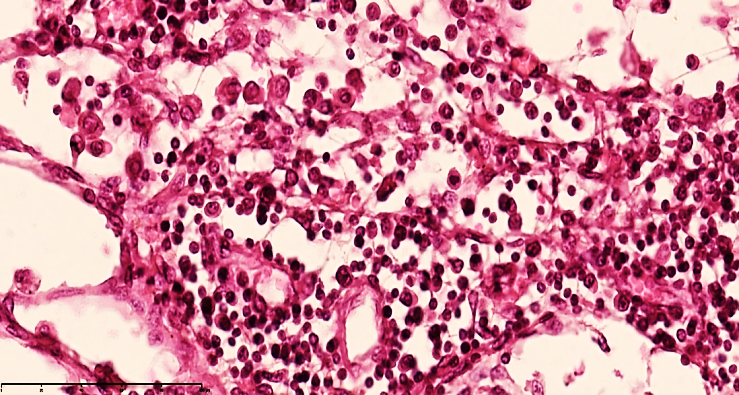
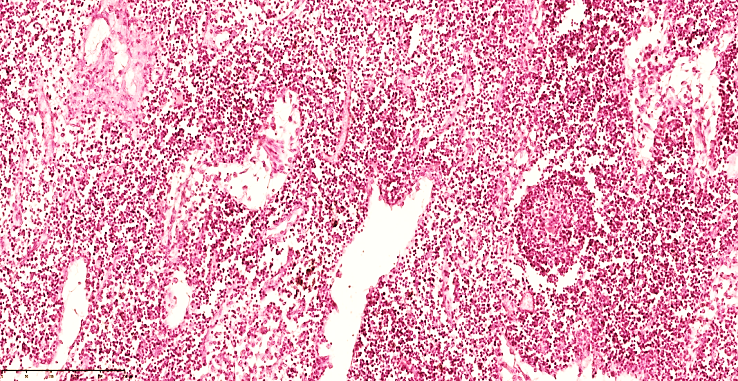
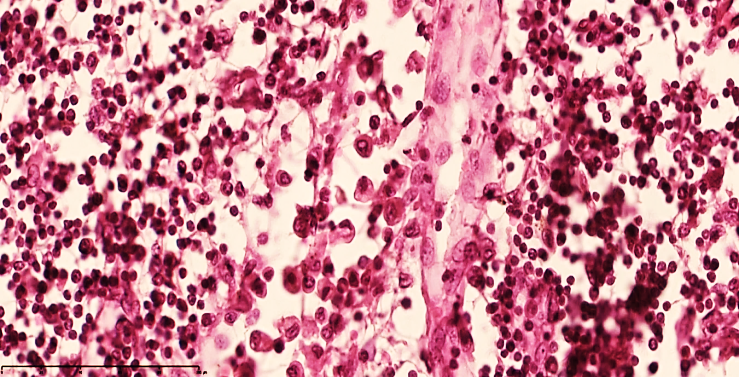 | Figure 3. Mesenteric lymph node of a 28-day-old infant with peritonitis. Macrophages are increased in the peritrabecular area, lymphocytes are decreased, and oligonucleated lymphoblasts are increased, and stroma is disrupted. Staining G.E. Size 40x10 |
 | Figure 4. Mesenteric lymph node of a 28-day-old infant with peritonitis. Treated on the 6th day. Macrophages increased in the peritrabecular area, lymphocytes and plasma cells decreased, and oligonucleated lymphoblasts increased, and stroma was found to be disrupted. Vascular dilation and collapse were detected. Staining G.E. Size 40x10 |
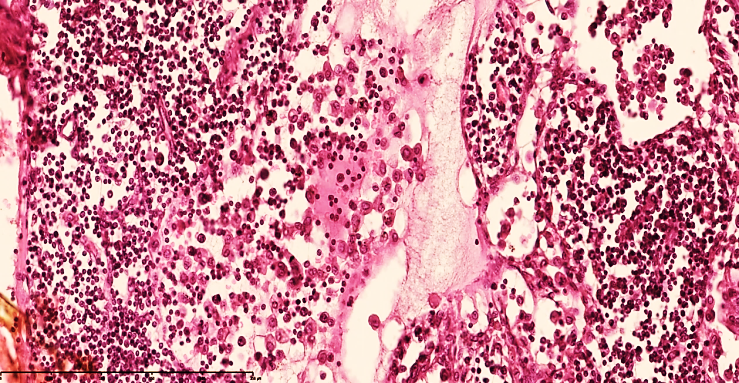
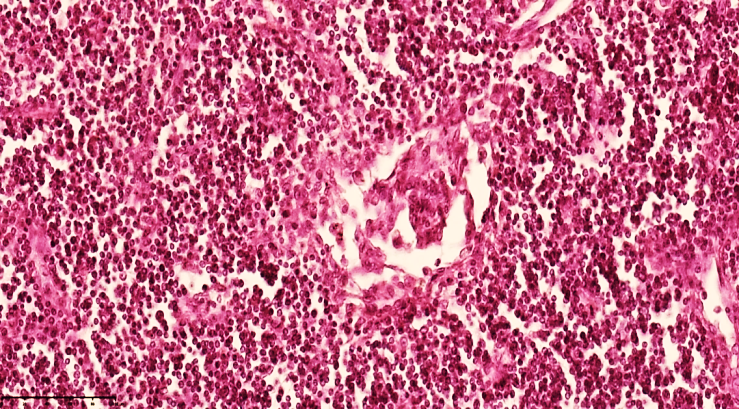
 | Figure 5. Mesenteric lymph node of a 28-day-old infant with peritonitis. In the cortical area, lymphocytes and plasma cells are reduced, lymphoblasts are increased with nucleoli, and stroma is disrupted. Delymphatic foci are detected. Staining G.E. Size 40x10 |
 | Figure 6. Mesenteric lymph node of a 28-day-old infant with peritonitis. Treated on the 3rd day. In the cortical area, lymphocytes and plasma cells are reduced, mononuclear lymphoblasts are increased, and stroma is disintegrated. In the form of a cone, foci of reticulocytosis are detected. Staining GE. Size 40x10 |
 | Figure 7. Mesenteric lymph node of a 28-day-old infant with peritonitis. Treated on the 13th day. Lymphocytes and plasma cells decreased in the cortical area, mononuclear lymphoblasts increased, and stroma wasting was detected. Delymphatic foci were detected. Staining G.E. Size 40x10 |
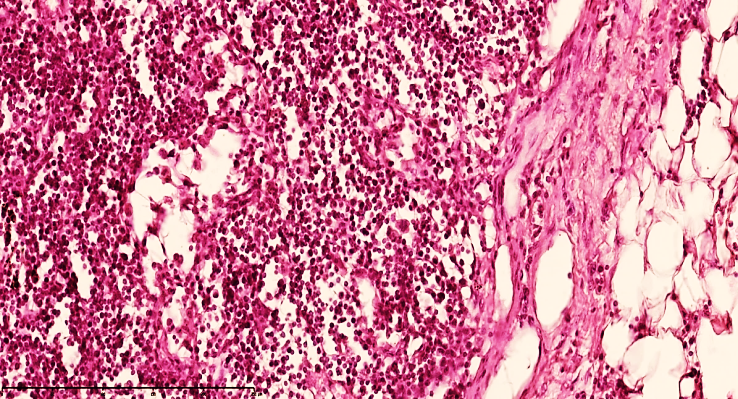 | Figure 8. Mesenteric lymph node of a 28-day-old infant with peritonitis. The capsule is markedly thickened, traces of lymphoid follicles are visible, and cystic spaces are formed in the space. Stained with GE. Size 40x10 |
 | Figure 9. Mesenteric lymph node of a 28-day-old infant with peritonitis. Treated on the 15th day. Fragmented capsule with cystic expansion in the space between. The boundaries of the cortex and medulla are determined. The main hypercellularity is formed by lymphoblasts. Staining G.E. Size 40x10 |
 | Figure 10. Mesenteric lymph node of a 28-day-old infant with peritonitis. In the corticomedullary area, there are scattered foci along the trabecular border, with the appearance of interstitial space.Stained with GE. Size 10x10 |
 | Figure 11. 28-day-old infant. Mesenteric lymph node of a 28-day-old infant with peritonitis. Single atrophic lymphoid follicles are detected in the cortex. A small number of macrophages and reticulocytes are detected in the germinal center. Most of the blood vessels are dilated, and foci of reticulocytosis are detected in the stroma. Staining G.E. Size 10x10 |
4. Conclusions
- In infants who died of peritonitis at the age of 28 days, a sharp decrease in lymphocytes, emptying of the sinuses, unclear boundaries between the cortex and medulla, lack of formation of lymphoid follicles, and accumulation of homogeneous protein substrates in the stroma of the lymph node, mainly consisting of macrophages, lymphoblasts, reticular cells, massive necrotic masses, are detected in the mesenteric lymph nodes. Blood vessels are unevenly filled, reticulocytosis, delymphatization and lymph node histioarchitectonic disorders were found.It is determined that symptoms of lymphangitis in lymph nodes and lymphadenitis in lymph nodes are preserved. The fact that the number of immunocompetent cells in the active areas of the lymph node has not yet fully occupied the lost volume and the presence of infiltrating foci of neutrophils and macrophages around the postcapillary venules requires the addition of other methods to the treatment tactics, requiring the protection of the parallel connection in the vein-lymph drainage system in the damaged areas.