-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(1): 275-280
doi:10.5923/j.ajmms.20261601.60
Received: Dec. 2, 2025; Accepted: Dec. 26, 2025; Published: Jan. 22, 2026

Outcomes of Periprosthetic Joint Infection of the Knee Joint After Two-Stage Revision Arthroplasty
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMurodulla Y. Karimov1, Umid T. Kholmurodov2, Javokhir Sh. Kayumov2
1MD, DSc, Professor, Head of the Department of Traumatology, Orthopedics and Military Field Surgery No.1, Tashkent State Medical University, Tashkent, Uzbekistan
2MD, PhD, Assistant Professor of the Department of Traumatology, Orthopedics and Military Field Surgery No.1, Tashkent State Medical University, Tashkent, Uzbekistan
Correspondence to: Murodulla Y. Karimov, MD, DSc, Professor, Head of the Department of Traumatology, Orthopedics and Military Field Surgery No.1, Tashkent State Medical University, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

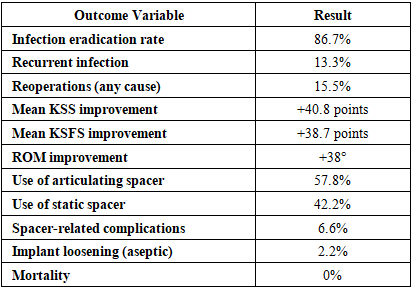
Background. Periprosthetic joint infection (PJI) after total knee arthroplasty (TKA) remains one of the most difficult complications to manage due to biofilm formation, antimicrobial resistance, and the need for complex revision surgery. Two-stage revision arthroplasty is widely regarded as the gold-standard treatment for chronic knee PJI, yet regional data from Central Asia remain limited. This study evaluates clinical, microbiological, and functional outcomes of two-stage revision for chronic knee PJI at a tertiary referral centre in Uzbekistan. Materials and Methods. A retrospective review was conducted of 45 consecutive patients with chronic knee PJI treated with a standardized two-stage revision protocol at Tashkent State Medical University between 2018 and 2023. Diagnosis was based on 2018 ICM criteria. All patients underwent explantation, radical debridement, antibiotic-loaded cement spacer placement, systemic pathogen-targeted antibiotic therapy, and subsequent reimplantation after clinical and laboratory normalization. Primary outcome was infection eradication at minimum 12-month follow-up. Secondary outcomes included Knee Society Score (KSS), Knee Society Functional Score (KSFS), range of motion (ROM), microbiological profile, and postoperative complications. Results. Infection eradication was achieved in 39 of 45 patients (86.7%) at a mean follow-up of 32.8 ± 10.4 months. Functional outcomes improved significantly, with mean KSS increasing from 38.6 ± 10.2 preoperatively to 79.4 ± 8.9 at final follow-up (p < 0.001), and KSFS from 34.1 ± 11.4 to 72.8 ± 10.6 (p < 0.001). ROM improved from 54° ± 18° to 92° ± 15° post-reimplantation (p < 0.001). Staphylococcal species were the predominant pathogens; culture-negative infection occurred in 24.4%. Complication rate was 22.2%, with recurrent infection in 13.3%, spacer-related issues in 6.6%, and no infection-related mortality. Conclusion. Two-stage revision arthroplasty remains a highly effective strategy for managing chronic knee PJI, providing high eradication rates and substantial functional recovery. Outcomes from this Central Asian cohort align with international data, demonstrating that rigorous adherence to established surgical and antibiotic protocols can ensure reliable results even in resource-limited settings. Further multicenter and prospective studies are required to refine protocols, incorporate advanced diagnostics, and assess long-term implant survival.
Keywords: Periprosthetic joint infection, Knee prosthesis, Arthroplasty, Treatment outcome
Cite this paper: Murodulla Y. Karimov, Umid T. Kholmurodov, Javokhir Sh. Kayumov, Outcomes of Periprosthetic Joint Infection of the Knee Joint After Two-Stage Revision Arthroplasty, American Journal of Medicine and Medical Sciences, Vol. 16 No. 1, 2026, pp. 275-280. doi: 10.5923/j.ajmms.20261601.60.
1. Introduction
- Periprosthetic joint infection (PJI) of the knee remains one of the most devastating complications following total knee arthroplasty (TKA). Although the incidence of infection after primary TKA is relatively low—estimated between 1.0% and 2.5%, depending on patient risk factors and institutional volume—its clinical and socioeconomic impact is profound [1,2]. PJI is associated with prolonged hospitalization, repeated surgical interventions, long-term functional impairment, and a dramatic decline in quality of life. Globally, PJI has emerged as the leading cause of revision TKA in the first two years after implantation and accounts for approximately 20–30% of all revision knee arthroplasties, underscoring its substantial clinical burden [3].The pathogenesis of PJI is multifactorial, typically involving bacterial adhesion to implant surfaces and subsequent biofilm formation, which renders microorganisms highly resistant to host immune mechanisms and systemic antibiotics. Staphylococcus aureus, coagulase-negative staphylococci, and gram-negative organisms represent the predominant pathogens in many cohorts. However, the growing prevalence of multidrug-resistant organisms (MDROs), polymicrobial infections, and culture-negative PJIs presents additional diagnostic and therapeutic challenges. These patterns vary substantially across geographic regions and reflect both the microbial ecology and local standards of surgical practice [4].Despite significant advances in diagnostics, including improved microbiological techniques and updated Musculoskeletal Infection Society (MSIS)/International Consensus Meeting (ICM) criteria, the management of knee PJI remains highly complex. A wide range of surgical strategies exist—irrigation and debridement, one-stage revision, two-stage revision, and, in severe cases, arthrodesis or amputation. Among these, the two-stage revision arthroplasty technique has historically been regarded as the gold standard in chronic PJI, with reported infection-eradication rates ranging from 70% to 95% in the literature [5]. This method includes prosthesis removal, aggressive debridement, placement of an antibiotic-loaded spacer, targeted parenteral antibiotic therapy, and subsequent reimplantation after infection control is achieved.Nevertheless, outcomes of the two-stage approach vary widely across institutions, influenced by patient comorbidities, microbial profile, compliance with treatment protocols, surgical technique, and postoperative rehabilitation. In low- and middle-income countries, including Uzbekistan, additional factors such as delays in diagnosis, limited access to advanced microbiological testing, and variability in antibiotic stewardship policies may further affect outcomes. Despite the high national prevalence of lower limb arthroplasties and the growing number of revision procedures, there remains a notable scarcity of region-specific clinical data from Central Asia—particularly from Uzbekistan—regarding epidemiological characteristics, microbial patterns, and treatment outcomes of knee PJI.Tashkent State Medical University (TSMU), as one of the largest tertiary-level orthopedic centers in Uzbekistan, manages a significant volume of complex infected arthroplasty cases, including PJIs requiring revision surgery. Understanding the outcomes of two-stage revision procedures performed in this clinical setting is essential not only to evaluate the effectiveness of local treatment protocols but also to contribute to the global body of evidence on PJI management.The present study analyzes 45 consecutive patients with chronic periprosthetic joint infection of the knee treated with two-stage revision arthroplasty at Tashkent State Medical University. The objective of this work is to assess infection-eradication rates, functional outcomes, microbiological characteristics, and complication profiles in this cohort. By providing a detailed clinical analysis within the regional context, this study aims to support future optimization of diagnostic pathways, perioperative protocols, antibiotic strategies, and surgical techniques in the treatment of knee PJI.
2. Materials and Methods
- This was a retrospective, single-center clinical study conducted at the Department of Traumatology and Orthopedics of Tashkent State Medical University, one of the largest national referral centers for arthroplasty and revision surgery in Uzbekistan. The study evaluated all patients who underwent two-stage revision arthroplasty for chronic periprosthetic joint infection (PJI) of the knee between January 2018 and December 2023. Ethical approval was obtained from the institutional review board of TSMU, and all patients provided informed consent for surgical treatment and the use of anonymized data for research purposes.Patients were eligible for inclusion if they met all of the following criteria:1. Diagnosis of chronic periprosthetic joint infection of the knee based on the 2018 International Consensus Meeting (ICM) criteria.2. Treatment with planned two-stage revision knee arthroplasty.3. Minimum follow-up period of 12 months after the second-stage reimplantation.4. Age ≥ 18 years.Patients were excluded if they had:• Acute postoperative infections (< 4 weeks following primary TKA) treated with debridement and implant retention (DAIR).• Incomplete medical records or loss to follow-up before the second-stage reimplantation.• Refusal or inability to undergo reimplantation (leading to permanent spacer, arthrodesis, or amputation).• Concomitant hip or ankle infections requiring additional interventions.A total of 45 patients met the inclusion criteria and were included in the analysis.All patients underwent standardized clinical evaluation including assessment of pain severity, joint swelling, erythema, presence of sinus tracts, local temperature, and range of motion.Baseline and pre-reimplantation laboratory investigations included:• C-reactive protein (CRP)• Erythrocyte sedimentation rate (ESR)• Serum leukocyte count and differential• Procalcitonin (in selected cases)Aspiration was performed in all patients before Stage 1 and before Stage 2. Analysis included:• Total leukocyte count• Polymorphonuclear neutrophil percentage (PMN%)• Aerobic and anaerobic cultures• Fungal cultures (in high-risk or recurrent cases)Synovial biomarkers such as α-defensin or leukocyte esterase were not universally available and thus used selectively.Standard anteroposterior and lateral knee radiographs were obtained prior to surgery, after spacer implantation, and after reimplantation. CT or MRI was performed only when needed to evaluate occult bone loss, soft-tissue compromise, or suspected sinus tracts.All patients underwent:1. Removal of all prosthetic components and cement.2. Radical debridement of infected and necrotic tissue.3. Pulsatile lavage with 6–9 liters of saline.4. Intramedullary canal reaming where indicated.5. Collection of at least five periprosthetic tissue samples for microbiology.Antibiotic-loaded cement spacers were used in all cases. Static spacers — used in cases of severe bone loss, ligament deficiency, or poor soft-tissue condition.Data were analyzed using SPSS version 26. Continuous variables were expressed as mean ± standard deviation or median with interquartile range, depending on distribution. Categorical variables were summarized as frequencies and percentages. Comparisons between pre- and postoperative variables were performed using paired t-tests or Wilcoxon signed-rank tests. Factors associated with reinfection were explored using logistic regression. Statistical significance was set at p < 0.05.
3. Results
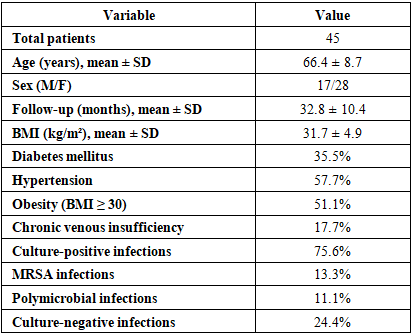
- A total of 45 patients (28 women, 17 men) with chronic periprosthetic joint infection (PJI) of the knee underwent a standardized two-stage revision protocol at Tashkent State Medical University. The mean age at Stage 1 was 66.4 ± 8.7 years (range 49–82). The average follow-up duration after reimplantation was 32.8 ± 10.4 months (range 12–60 months). All patients completed the full two-stage protocol.The most common comorbidities included obesity (51.1%), type 2 diabetes mellitus (35.5%), hypertension (57.7%), and chronic venous insufficiency (17.7%). Despite the presence of multiple risk factors, the majority of patients demonstrated favorable recovery and infection control following treatment (Table 1).
|
|

|
4. Discussion
- This study presents the mid-term outcomes of 45 patients with chronic periprosthetic joint infection (PJI) of the knee treated with a standardized two-stage revision protocol at a high-volume tertiary center in Uzbekistan. The principal findings are: (1) an infection-eradication rate of 86.7%, which lies within the upper range of success rates reported for two-stage revision in the international literature; (2) substantial functional improvement, with mean KSS and KSFS nearly doubling from baseline; and (3) a low rate of major complications and no infection-related mortality over a mean follow-up of almost three years. Taken together, these results support the effectiveness and safety of two-stage revision as the preferred strategy for chronic knee PJI in our regional context.Two-stage revision remains widely regarded as the “gold standard” for chronic PJI of the hip and knee, with infection-free survival typically reported between 80% and 90% in large series and systematic reviews [6,7]. Our eradication rate of 86.7% aligns closely with these benchmarks and is very similar to recent large studies reporting success rates of 83–88% after two-stage exchange [8]. Contemporary registry and cohort data also show that two-stage revision provides comparable or superior implant survival relative to other strategies such as debridement-and-retention or one-stage exchange, particularly in chronic or complex infections [5]. The fact that our outcomes are consistent with high-volume centers in Europe and North America suggests that a carefully implemented two-stage protocol can deliver reliable results even in a resource-constrained setting.From a functional standpoint, our patients experienced a marked and clinically meaningful improvement. The mean KSS increased from approximately 39 to 79 points and the functional score from 34 to 73, with range of motion improving by nearly 40°. These gains are highly comparable to other two-stage series, in which postoperative KSS values typically range from 75 to 85 and ROM averages around 90–100° [9].Importantly, our final scores fall within the range reported after revision for non-infective indications, highlighting that eradication of infection does not need to come at the expense of acceptable function. Nonetheless, it should be acknowledged that functional outcomes after PJI revision rarely match those after uncomplicated primary TKA, and patients should be counseled accordingly. Our microbiological findings mirror global trends while also reflecting local features. Staphylococcal species—particularly Staphylococcus aureus and coagulase-negative staphylococci—were the dominant pathogens, consistent with their role as the most common causative organisms in knee PJI worldwide [10].The presence of methicillin-resistant S. aureus (MRSA) in more than 10% of cases and a notable proportion of gram-negative and polymicrobial infections underlines the importance of robust microbiological workup and close collaboration with infectious disease specialists. Our culture-negative rate of 24.4% is higher than some Western series but similar to other reports that used prior or prolonged empirical antibiotics; it may also reflect limitations in routine culture techniques and availability of advanced diagnostics such as sonication or molecular assays in our context [11]. Despite this, infection control in culture-negative cases was acceptable, suggesting that aggressive debridement combined with broad-spectrum and then rationally narrowed systemic therapy can still be effective where sophisticated microbiology is not universally available.The reinfection rate of 13.3% is in line with published reinfection or failure rates after two-stage knee revision, which range from 10% to 20% in many modern series [10,12].Long-term studies have shown that failures can continue to accrue over time, particularly beyond five years, and that mortality after PJI revision can approach 15–30% at extended follow-up [2,13]. Our mean follow-up of roughly 33 months and absence of infection-related death are therefore encouraging but should be interpreted cautiously; further follow-up is required to confirm long-term durability of infection control and implant survival. An interesting observation in our cohort was the functional advantage of articulating spacers compared with static spacers, without a measurable difference in infection-eradication rates. This finding is concordant with previous reports that articulating spacers can facilitate preservation of soft tissue tension, reduce stiffness, and improve ROM at final follow-up, while maintaining comparable infection control to static designs.In our practice, static spacers were reserved for patients with major bone loss, ligamentous insufficiency, or compromised soft tissues. This selection bias likely explains part of the functional gap between groups; nonetheless, the overall message is that, where feasible, articulating spacers should be preferred to optimize postoperative mobility and rehabilitation. Our study also adds important data from a Central Asian setting, where published evidence on PJI management remains sparse. The burden of comorbidities in our cohort—over half of patients obese and one-third diabetic—is comparable to that reported in Western series, suggesting that the risk profile of revision populations is converging globally [11,14].However, regional differences in antibiotic availability, stewardship policies, and microbiologic infrastructure may shape outcomes. For instance, delayed referral, prior prolonged antibiotic courses in community settings, and limited access to advanced imaging or intraoperative diagnostics can complicate diagnosis and targeted therapy. Demonstrating outcomes that match international benchmarks under these circumstances is therefore particularly relevant for similar health systems in low- and middle-income countries.When comparing two-stage revision to alternative strategies, current literature suggests that one-stage exchange may achieve comparable infection control in carefully selected patients with known, susceptible organisms, good soft-tissue envelope, and absence of sinus tracts [7].However, two-stage remains the most widely used and best validated approach for chronic or complex PJI, particularly in cases with resistant or polymicrobial infections, uncertain microbiology, or prior failed procedures [15]. In our center, most patients presented late and often after prior interventions, making them less suitable for one-stage exchange based on current consensus criteria. As diagnostic capabilities and multidisciplinary infrastructure mature, selective use of one-stage exchange in low-risk cases may reduce overall treatment burden, but robust patient-selection algorithms and local outcome data will be essential before shifting practice. Several factors have been identified in the literature as predictors of failure after two-stage revision, including poor host status, severe local soft-tissue compromise, resistant organisms, multiple previous surgeries, and repeated spacer exchanges [10,12].Although our sample size was limited for detailed multivariable modeling, most failures occurred in patients with substantial comorbidity or challenging local conditions. This is in line with reports that emphasize the Musculoskeletal Infection Society (MSIS) host and extremity grades as powerful prognostic indicators [10]. The implication for clinical practice is that early referral, optimization of systemic risk factors, and careful handling of soft tissues remain cornerstones of successful PJI management. Additionally, avoiding unnecessary intermediary spacer exchanges and standardizing antibiotic protocols may reduce the risk of selecting for resistant flora and improve outcomes. Our findings have important practical implications for orthopedic practice in Uzbekistan and similar settings. First, they support the continued use of a structured two-stage protocol with rigorous debridement, systematic tissue sampling, articulating spacers where feasible, and close infectious disease collaboration. Second, they highlight the need to strengthen microbiology services, including implementation of extended culture techniques and, where possible, sonication or molecular diagnostics to reduce culture-negative rates and refine antibiotic strategies. Third, they underscore the importance of multidisciplinary perioperative care—endocrinology, cardiology, rehabilitation—to optimize host status and functional recovery in this frail patient population.This study has several limitations that warrant discussion. Its retrospective design inherently introduces potential selection and information bias. All procedures were performed at a single tertiary institution, which may limit generalizability but also ensures consistency of surgical technique and postoperative management. The sample size of 45 patients, although comparable to many single-center PJI series, restricts the power to detect smaller differences and to perform robust multivariate analyses of risk factors for failure. Follow-up, while sufficient to capture early and mid-term failures, may still underestimate late reinfections or aseptic failures that emerge beyond five years. Moreover, we relied primarily on traditional outcome measures (KSS, KSFS, ROM) and did not systematically collect patient-reported outcome measures (PROMs) such as the WOMAC or EQ-5D, which are increasingly recognized as critical for assessing the broader impact of complex revision surgery on quality of life [7,14]. Finally, the absence of advanced diagnostics (e.g., synovial biomarkers for all patients, next-generation sequencing) might have contributed to the relatively high culture-negative rate and limited our ability to characterize low-grade infections.Despite these limitations, our study has notable strengths. It represents one of the first detailed series from Uzbekistan focusing specifically on chronic knee PJI treated by two-stage revision, with a clearly defined surgical protocol and minimum 12-month follow-up after reimplantation. The cohort is homogeneous in terms of indication (all chronic PJI), procedure (all two-stage revisions), and institutional practice, allowing a focused evaluation of outcomes. The comprehensive assessment of clinical, microbiological, and functional parameters provides a realistic picture of what can be achieved in a tertiary orthopedic center in a middle-income country when evidence-based protocols are consistently applied.Future research should aim to expand the cohort, extend follow-up to capture long-term implant survival and mortality, and integrate more sophisticated microbiological and biomarker diagnostics. Prospective multicenter collaboration within Uzbekistan and across Central Asia would help validate our findings, allow comparison of one-stage and two-stage strategies in carefully selected groups, and support the development of regional guidelines for PJI management. Incorporating standardized PROMs and cost-effectiveness analyses would further clarify the overall value of different approaches in health systems with constrained resources.In summary, our data confirm that two-stage revision arthroplasty provides high rates of infection eradication and meaningful functional recovery in patients with chronic knee PJI treated at Tashkent State Medical University. These outcomes are comparable to those reported in high-income countries and underscore the feasibility and effectiveness of a structured, multidisciplinary approach to PJI within our regional context.
5. Conclusions
- In this cohort of 45 patients with chronic periprosthetic joint infection of the knee treated with a standardized two-stage revision protocol at Tashkent State Medical University, we observed an infection-eradication rate of 86.7% and substantial functional gains, with no infection-related mortality over a mean follow-up period of approximately 33 months. These results compare favourably with those reported in international series and demonstrate that a well-structured two-stage revision strategy can achieve robust outcomes even in a middle-income, regional orthopaedic centre. The findings underscore the importance of comprehensive debridement, judicious use of antibiotic-loaded spacers (preferably articulating when feasible), multidisciplinary coordination (including infectious disease, rehabilitation, and medical risk-factor optimisation), and rigorous monitoring prior to reimplantation.Nevertheless, given the inherent complexity of knee PJI, further work is needed to refine patient selection, standardise intra- and inter-stage protocols, adopt advanced microbiological diagnostics to reduce culture-negative cases, and extend follow-up to capture long-term implant survival and functional durability. Ultimately, region-specific outcome data such as this study serve as a foundation for improving PJI care pathways and may help to reduce the morbidity, cost and resource burden associated with knee PJI in Central Asia and similar health-care environments.