-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(1): 258-262
doi:10.5923/j.ajmms.20261601.57
Received: Nov. 24, 2025; Accepted: Dec. 16, 2025; Published: Jan. 22, 2026

Ischemic Stroke: Age-Related Clinical and Morphological Features and Therapeutic Effectiveness
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSharofiddinov Kamoliddin1, Musaeva Yulduz2
1Assistant, Tashkent State Medical University Termez Branch, Surkhandaryo, Uzbekistan
2Associate Professor, Tashkent State Medical University, Tashkent, Uzbekistan
Correspondence to: Sharofiddinov Kamoliddin, Assistant, Tashkent State Medical University Termez Branch, Surkhandaryo, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This article presents the results of a comprehensive morphological, histochemical, morphometric, and immunohistochemical study of the brain in individuals who died from ischemic stroke. The research was based on 64 autopsy cases conducted at the Republican Center of Pathological Anatomy during 2022–2024. The main focus is on age and gender differences in the incidence of stroke, duration of hospitalization, pathomorphological changes in brain tissue, and concomitant somatic diseases contributing to the development of cerebrovascular catastrophes. It was found that the highest frequency of fatal outcomes occurred in the age group of 69–88 years (54.6% of all cases), predominantly among women (57.8%). The leading concomitant diseases were arterial hypertension (23.4%), diabetes mellitus (21.9%), and atherosclerosis (11.0%), which formed the basis of vascular-degenerative changes in the brain tissue. Morphological, histochemical, and immunohistochemical data made it possible to identify the key pathogenetic mechanisms of ischemic injury: neuronal necrosis, gliosis, vasogenic edema, disruption of the blood-brain barrier, microglial activation, and apoptosis. A correlation was established between the severity of these changes, age, and the duration of the disease.
Keywords: Ischemic stroke, Cerebrovascular diseases, Morphological changes, Histochemistry, Immunohistochemistry, Gliosis, Apoptosis, Age-related features, Arterial hypertension, Brain
Cite this paper: Sharofiddinov Kamoliddin, Musaeva Yulduz, Ischemic Stroke: Age-Related Clinical and Morphological Features and Therapeutic Effectiveness, American Journal of Medicine and Medical Sciences, Vol. 16 No. 1, 2026, pp. 258-262. doi: 10.5923/j.ajmms.20261601.57.
Article Outline
1. Introduction
- Ischemic stroke remains one of the leading causes of mortality and disability worldwide, ranking second among all causes of death after cardiovascular diseases. According to the World Health Organization, more than 15 million stroke cases are recorded annually, of which about 5 million are fatal, and another 5 million result in permanent disability [1,2,3,4,5,6].In the structure of cerebrovascular diseases (CVD), ischemic forms account for up to 80–85% of all cases. Despite the advances in modern medicine, including the use of thrombolytic therapy, anticoagulants, and intensive care methods, the mortality rate from ischemic stroke remains high, particularly among older age groups [7,8,9,10].Age and gender characteristics play a decisive role in the clinical course and outcomes of ischemic stroke. It is known that men often develop the disease at a younger age; however, in women- especially after menopause- a more severe course and higher mortality rate are observed. Hormonal changes, decreased estrogen protection, and the combination of chronic somatic pathologies such as hypertension, diabetes mellitus, and atherosclerosis increase the risk of fatal complications [11].From a morphological point of view, ischemic stroke represents a complex cascade of biochemical and cellular processes, including neuronal energy depletion, activation of apoptosis, disruption of the blood-brain barrier, development of vasogenic and cytotoxic edema, and formation of gliosis. Understanding these changes in relation to the patient’s age is of great importance for improving therapeutic strategies and predicting the outcome of the disease [12,13].In domestic pathomorphological practice, the age-related aspects of ischemic stroke have not been sufficiently studied. Meanwhile, a detailed investigation of the morphofunctional changes in brain tissue accompanying ischemia opens new opportunities for clinical and pathogenetic analysis and for the implementation of a personalized approach in the treatment of patients with cerebrovascular pathology.The study of age-related clinical and morphological features of ischemic stroke is a relevant area of modern neuromorphology, aimed at improving the effectiveness of diagnosis, treatment, and prevention of cerebrovascular catastrophes [14,15].
2. Purpose of the Study
- The aim of the present research was to identify and perform a comparative analysis of age-related clinical, morphological, morphometric, and immunohistochemical features of ischemic stroke, as well as to assess their relationship with concomitant diseases and the duration of hospitalization.To achieve the stated goal, the following objectives were defined:1. To analyze the incidence of ischemic stroke by age and gender groups among deceased individuals.2. To study clinical, laboratory, and autopsy data reflecting the course of the disease and causes of death.3. To conduct a comprehensive morphological examination of the brain, including histological, histochemical, and immunohistochemical methods.4. To determine the nature and degree of severity of pathomorphological changes depending on age, gender, and duration of the disease.5. To assess the impact of concomitant somatic diseases on the outcome of ischemic stroke.6. Based on the obtained data, to develop morphological criteria for assessing the severity of ischemic brain damage.
3. Materials and Methods
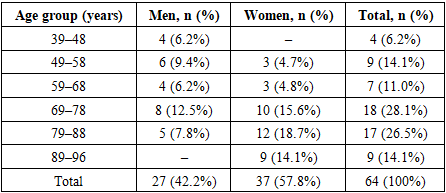
- The material for this study consisted of autopsy data from 64 deceased individuals with clinically and morphologically confirmed cases of ischemic stroke, performed at the Republican Center of Pathological Anatomy during the period from 2022 to 2024. All cases were documented in accordance with current ethical and legal standards.Of the total number of examined individuals, 27 (42.2%) were men and 37 (57.8%) were women. The age of the subjects ranged from 39 to 96 years. For analytical purposes, six age groups were identified:• Group I: 39–48 years — 4 cases (6.2%)• Group II: 49–58 years — 9 cases (14.1%)• Group III: 59–68 years — 7 cases (11.0%)• Group IV: 69–78 years — 18 cases (28.1%)• Group V: 79–88 years — 17 cases (26.5%)• Group VI: 89–96 years — 9 cases (14.1%)The highest frequency of fatal ischemic stroke was observed in the age range of 69–88 years (54.6%), predominantly among women.Analysis of clinical case histories showed that the duration of hospitalization ranged from less than one day to 15 days. Within the first 24 hours after admission, 18 patients (28.1%) died; between 2 and 3 days — 17 cases (26.6%); between 4 and 7 days — 15 cases (23.4%); and between 8 and 15 days — 14 cases (21.9%).Nearly one-third of patients died within the first 24 hours after hospitalization, which indicates an extremely severe course of the disease, delayed seeking of medical care, and insufficient effectiveness of emergency therapy.To achieve the objectives of the study, a comprehensive set of morphological, histological, histochemical, morphometric, and immunohistochemical methods was applied.Macroscopic and microscopic changes in brain tissue were studied, including neuronal, glial, and vascular structures. Tissue samples were fixed in 10% neutral formalin, dehydrated using the standard ascending alcohol concentration technique, and embedded in paraffin. Histological sections 4–5 μm thick were stained with hematoxylin and eosin, Van Gieson’s stain, and Schiff’s reagent (PAS reaction).Reactions were used to identify structural and biochemical changes: Nissl staining - for the assessment of neuronal chromatolysis; determination of acid and alkaline phosphatase activity; Perls’ reaction — for the detection of hemosiderin and hemorrhagic transformations; PAS reaction — for visualization of glycoproteins and blood-brain barrier disruption; GFAP staining — for the evaluation of reactive gliosis.Morphometric measurements were carried out on digital images of micropreparations using the NanoZoomer system (Hamamatsu, Japan) and QuPath 0.4.0 software. Quantitative parameters were evaluated, including neuronal and glial cell density (in N/mm²), capillary diameter, perivascular space, and the area and volume of necrotic foci. The data were processed using methods of variation statistics, with the calculation of the arithmetic mean (M), standard deviation (σ), and level of significance (p).Immunohistochemistry was performed on paraffin sections using monoclonal antibodies against key protein markers: NeuN — for assessing neuronal preservation; GFAP — for reactive gliosis; Iba-1 — for microglial activation; Caspase-3 — for neuronal apoptosis; HIF-1α — for hypoxic activation; VEGF — for angiogenesis; and CD3 and CD20 — for evaluating lymphocytic infiltration.Visualization was performed using the DAKO LSAB2 Kit, with antibody incubation carried out at 37°C for 1–2 hours. The results were evaluated semi-quantitatively (based on the staining intensity scale) and by calculating the percentage of positively stained cells.
4. Results
- Among the 64 examined cases of ischemic stroke, 57.8% occurred in women and 42.2% in men. The highest number of deaths was observed in individuals aged 69–88 years, accounting for a total of 35 cases (54.6%). In the younger age groups (under 48 years), stroke was rare — only 4 cases (6.2%) (Table 1).
|
 | Diagram 1 |
5. Discussion
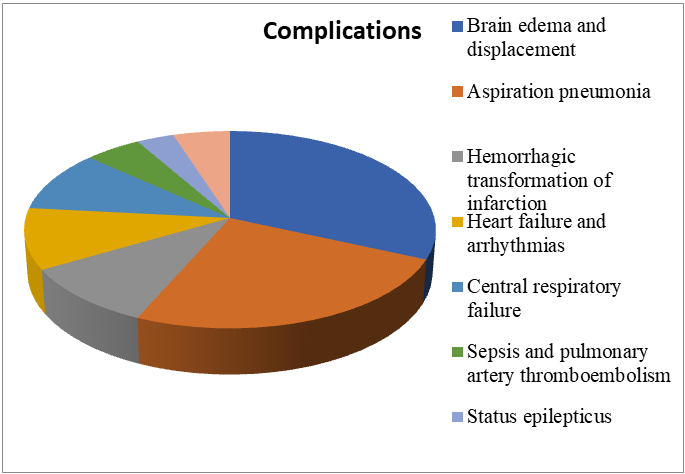
- The comprehensive morphological, histochemical, and immunohistochemical study of the brain in cases of ischemic stroke made it possible to identify consistent age-related and clinico-morphological features of this condition. The obtained results deepen the understanding of the pathogenesis of cerebrovascular disorders and hold significant importance for clinical neurology and pathomorphology. The incidence of fatal ischemic stroke increases proportionally with age. The highest mortality rates were observed in the age groups 69–78 years (28.1%) and 79–88 years (26.5%), which are associated with pronounced age-related changes in the vascular wall, atherosclerotic arterial lesions, and a decline in the body's compensatory capabilities. Among the deceased, women predominated (57.8%), reflecting the influence of postmenopausal hormonal changes, longer life expectancy, and the accumulation of chronic somatic diseases. In men, stroke more often developed at a younger age (39–68 years), frequently presenting acutely and malignantly, with a short interval between disease onset and fatal outcome.Nearly one-third of the patients (28.1%) died within the first 24 hours after hospital admission, indicating an extremely rapid progression of the ischemic process, delayed presentation for medical care, and the presence of severe forms of the disease.Patients who died within 4–15 days generally exhibited a more prolonged course of stroke, accompanied by the development of complications such as infections, cerebral edema, and multiple organ failure. The most significant underlying pathologies were arterial hypertension (23.4%), diabetes mellitus (21.9%), atherosclerosis (11.0%), as well as coronary heart disease and metabolic syndrome. The presence of these conditions creates a chronic angiopathic background that contributes to impaired microcirculation, thrombogenesis, and reduced vascular reactivity. The combination of several somatic disorders significantly aggravates the course of stroke, accelerating the development of cerebral edema and necrosis.The morphological pattern of ischemic stroke changes progressively over time:Early period (0–6 hours) — stage of cytotoxic edema, appearance of “red neurons,” vascular stasis;Acute period (6–24 hours) — neuronal necrosis, disruption of the blood-brain barrier, development of vasogenic edema;Subacute period (2–5 days) — activation of microglia and macrophages, onset of gliosis, demyelination;Chronic period (1–4 weeks) — formation of a cystic-gliotic focus, vascular hyalinosis, and astrocyte proliferation.The predominant type of brain lesion was ischemic infarction with perifocal gliosis and a penumbra zone, reflecting the heterogeneity of blood supply and the variability of ischemic damage.Ischemic stroke is accompanied by profound biochemical disturbances, including decreased activity of antioxidant enzymes (superoxide dismutase, catalase), accumulation of lipid peroxidation products, and disruption of membrane structure. The PAS reaction revealed destruction of basement membranes and increased vascular wall permeability, indicating the breakdown of the blood-brain barrier. Enhanced GFAP expression indicates the development of reactive gliosis as a compensatory response to neuronal death. Immunohistochemical studies revealed significant differences in the expression of protein markers depending on the duration of ischemia: NeuN — decreased number of viable neurons in the necrotic zone; Caspase-3 — marked activation of apoptosis in the affected areas; HIF-1α — intense hypoxic response, particularly in the penumbra zone; Iba-1 and CD68 — activation of microglia and macrophages, reflecting the inflammatory response; GFAP — enhanced astrocytic reaction leading to the formation of a glial scar; CD3 and CD20 — lymphocytic infiltration confirming the involvement of the immune component in brain tissue damage.The obtained data demonstrate that the pathogenesis of ischemic stroke is multifactorial, involving necrosis, apoptosis, inflammation, glial response, and microangiopathy.Quantitative analysis revealed a significant (p<0.05) decrease in neuronal density within the infarct zone by 45–60% compared to intact tissue. The gliosis index increased by an average of 70%, indicating a pronounced reactive proliferation of glial cells. The diameter of capillaries in the ischemic area was reduced by 25–30%, while perivascular spaces nearly doubled in size, correlating with the severity of vasogenic edema. In older patients, more pronounced enlargement of perivascular spaces and reduction of the microvascular network were observed, confirming the age-dependent nature of morphological changes.The observed morphological and immunohistochemical changes reflect the universal mechanisms of ischemic injury: energy deficiency, oxidative stress, apoptosis, and inflammation. In elderly and senile individuals, these processes are more pronounced due to reduced antioxidant activity, endothelial dysfunction, and structural degradation of the vascular wall. The study results emphasize the importance of early diagnosis and individualized stroke therapy, taking into account age, sex, and underlying comorbidities.
6. Conclusions
- Ischemic stroke is a complex multifactorial pathological process based on impaired cerebral circulation, accompanied by neuronal death, activation of glial elements, and structural remodeling of blood vessels.The conducted study demonstrated that: the patient’s age and sex are determining factors in disease outcome; the morphological severity of lesions directly correlates with the presence of underlying somatic pathologies; and the use of comprehensive methods — morphological, morphometric, histochemical, and immunohistochemical — allows for an objective assessment of the stage and extent of ischemic brain damage.The practical significance of the obtained data lies in the possibility of: differential diagnosis of ischemic stroke stages based on morphological criteria; prediction of disease outcome according to the severity of gliosis and apoptotic changes; and improvement of therapeutic and preventive approaches, taking into account age-related and pathogenetic factors.A comprehensive morphofunctional analysis of the brain in cases of ischemic stroke not only enables clarification of the causes of death but also facilitates the development of strategies to enhance the effectiveness of pathogenetic therapy and the rehabilitation of patients with cerebrovascular pathology.