-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(1): 252-257
doi:10.5923/j.ajmms.20261601.56
Received: Nov. 3, 2025; Accepted: Dec. 6, 2025; Published: Jan. 22, 2026

A Comparative Study of Surgical Techniques for Hemivertebra Treatment in Children: Resection Versus Decancellation
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLDjurayev Akhror Makhmudovich1, Kholov Zafar Soliyevich2, Kholboyev Golib Turg’un ugli3
1Prof. Head of the Department of Pediatric Orthopedics, Republican Specialized Scientific and Practical Medical Center for Traumatology and Orthopedics of Uzbekistan
2Ph.D., Specialist Traumatologist Orthopedist in the Department of Pediatric Orthopedics, Republican Specialized Scientific and Practical Medical Center for Traumatology and Orthopedics of Uzbekistan
3Specialist Traumatologist-Orthopedist in the Department of Pediatric Orthopedics, Republican Specialized Scientific and Practical Medical Center for Traumatology and Orthopedics of Uzbekistan
Correspondence to: Djurayev Akhror Makhmudovich, Prof. Head of the Department of Pediatric Orthopedics, Republican Specialized Scientific and Practical Medical Center for Traumatology and Orthopedics of Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background: Congenital scoliosis (CS) is a spinal deformity caused by vertebral malformations, often due to asymmetric growth of the spine. Hemivertebra (HV) is the most common vertebral anomaly in CS, leading to progressive spinal deformity. Surgical treatments, such as hemivertebra resection and decancellation, are used to correct these deformities. This study compares the outcomes of these two surgical techniques in pediatric patients with congenital scoliosis. Methods: A retrospective study was conducted at the Republican Specialized Scientific and Practical Medical Center of Traumatology and Orthopedics of Uzbekistan between 2021 and 2023. A total of 100 children with congenital scoliosis were included, with 70 active hemivertebra cases treated surgically. The patients were divided into two groups: Group A (n = 25) underwent hemivertebra resection, and Group B (n = 25) underwent hemivertebra decancellation. Preoperative and postoperative radiographic and MRI evaluations were performed to assess deformity correction. Results: Both resection and decancellation methods showed nearly identical outcomes in deformity correction, with significant improvement in scoliosis and kyphosis. Three years postoperatively, both groups demonstrated stability in the correction of spinal deformities. The resection group achieved a high degree of correction, but the decancellation group had less intraoperative blood loss, shorter operative time, and reduced risk of complications. Both techniques showed comparable long-term outcomes in terms of correction and stability of the deformity. Conclusion: The study concluded that partial decancellation of the hemivertebra is just as effective as resection in correcting congenital scoliosis, with the added benefits of reduced intraoperative trauma and blood loss. Given these advantages, decancellation can be recommended as a viable alternative surgical option for treating congenital scoliosis, particularly in children at higher risk for surgical complications.
Keywords: Congenital Scoliosis, Hemivertebra, Hemivertebra Resection, Hemivertebra Decancellation, Pediatric Spinal Deformity, Surgical Outcomes, Deformity Correction
Cite this paper: Djurayev Akhror Makhmudovich, Kholov Zafar Soliyevich, Kholboyev Golib Turg’un ugli, A Comparative Study of Surgical Techniques for Hemivertebra Treatment in Children: Resection Versus Decancellation, American Journal of Medicine and Medical Sciences, Vol. 16 No. 1, 2026, pp. 252-257. doi: 10.5923/j.ajmms.20261601.56.
1. Introduction
- Congenital scoliosis (CS) is a spinal deformity caused by structural defects in the vertebral column that emerge during embryogenesis. The primary driver of the condition is asymmetrical spinal growth, most commonly linked to vertebral malformations. The established nosology categorizes CS into three principal groups: formation defects, segmentation defects, and mixed anomalies [1,2]. The most prevalent formation defect is the hemivertebra (HV), an anomaly characterized by one-half of a vertebral body, a single pedicle, and its corresponding hemilamina [3]. The widely adopted McMaster and David classification further specifies HV types as fully segmented, partially segmented (semi-segmented), and unsegmented [4].The exact etiology of CS remains unclear, but a potential genetic basis is suggested, with a 5–10% risk of CS reported in siblings of affected individuals. Associated systemic anomalies are frequently observed, with genitourinary anomalies in 6% of patients and cardiovascular abnormalities in 15%. Occult intraspinal anomalies, particularly diastematomyelia, are seen in approximately 15% of cases. Hemivertebra is the most common vertebral anomaly, accounting for 45% of cases, and the most frequent pattern of spinal curvature is a right-sided thoracolumbar curve.The progression of scoliosis caused by HV varies widely, from 1° to 33° per year, depending on the type, location, and number of hemivertebrae [4,5]. Fully segmented HVs are more likely to cause progressive deformities, often requiring early surgical intervention [4,6]. Resection combined with instrumentation has been shown to be an effective treatment method [7–12], and early HV resection is increasingly being performed even in juvenile and infant patients [13–15].However, it is important to recognize that surgical management is not invariably required. Certain deformities caused by a solitary hemivertebra (HV) can exhibit long-term stability with little change during growth and surveillance [4,16]. Winter et al. even reported instances of spontaneous correction in patients with HV-related congenital scoliosis under prolonged observation [17]. In cases where the deformity shows slow or negligible progression, a strategy of vigilant monitoring is considered a valid therapeutic approach. The embryological basis of HVs lies in unilateral somite development failure. The ultimate severity of the resulting spinal curvature is largely dictated by the degree of compensatory formation in the contralateral vertebral body [18,19].
2. Materials and Methods
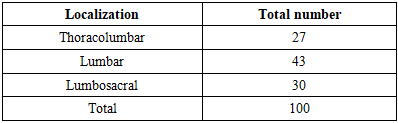
- A retrospective study was conducted at the Republican Specialized Scientific and Practical Medical Center of Traumatology and Orthopedics of Uzbekistan between 2021 and 2023. The aim was to compare the outcomes of hemivertebra resection and decancellation in pediatric patients with congenital scoliosis.Patient SelectionA total of 100 children aged 1 to 18 years with congenital scoliosis were included in the study. The cohort consisted of 62 girls (62%) and 38 boys (38%). Inclusion criteria were: Radiographically confirmed congenital scoliosis due to a hemivertebra; minimum follow-up period of 3 year. Exclusion criteria included patients with multiple vertebral anomalies or incomplete follow-up data.Patient GroupsOut of 100 patients, 30 were treated conservatively due to an inactive hemivertebra in an unsegmented formation. The remaining 70 patients had an active hemivertebra. Children under 5 years old with an active hemivertebra underwent combined approach hemivertebra extirpation (n = 20). Patients older than 5 years presented later with developed spinal deformities. These patients were divided into two groups based on the surgical technique used: Group A (n = 25): Posterior hemivertebra resection with transpedicular fixation; Group B (n = 25): Posterior hemivertebra decancellation with transpedicular fixation. All patients underwent radiographic evaluation as part of their preoperative assessment. In addition, magnetic resonance imaging (MRI) and multi-slice computed tomography (MSCT) were performed to evaluate the structural anomalies, assess the spinal deformities, and guide the surgical decision-making process.
|
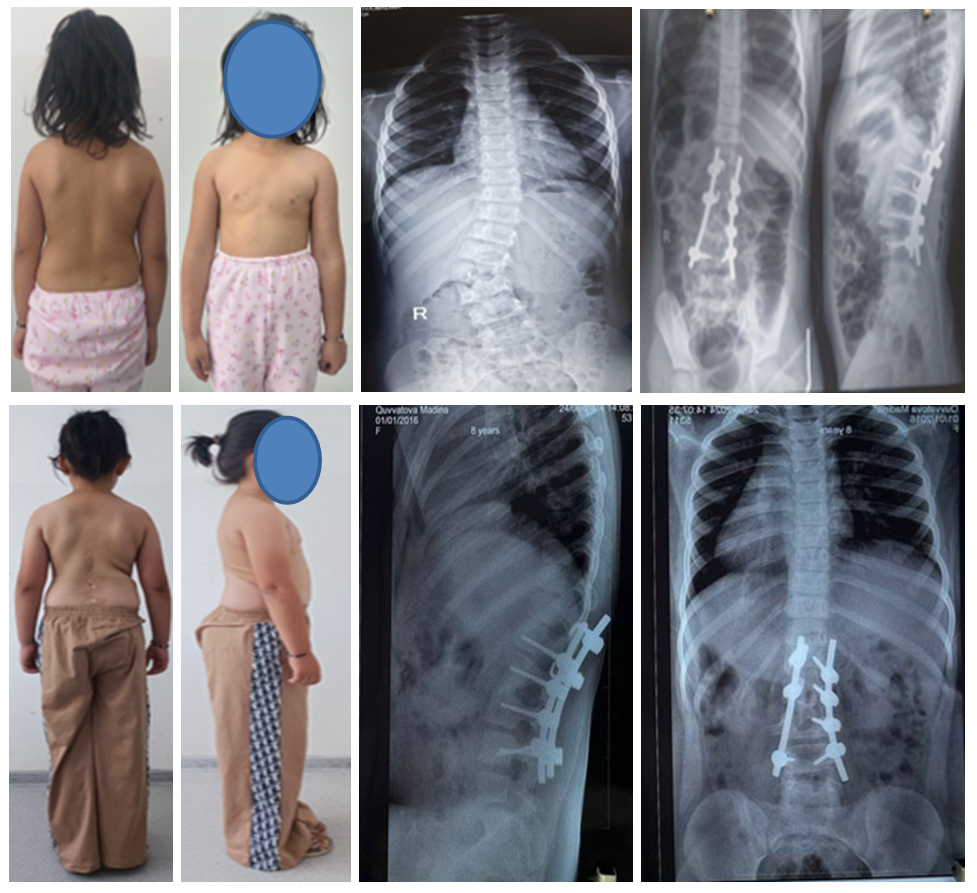 | Figure 1 |
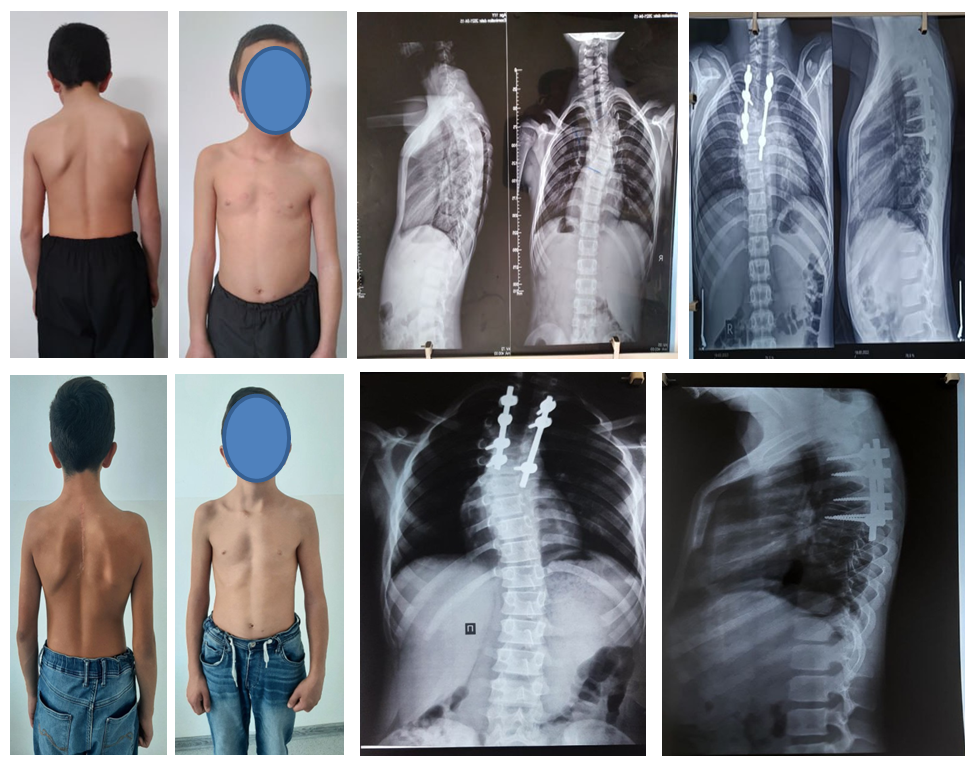 | Figure 2 |
|
3. Results
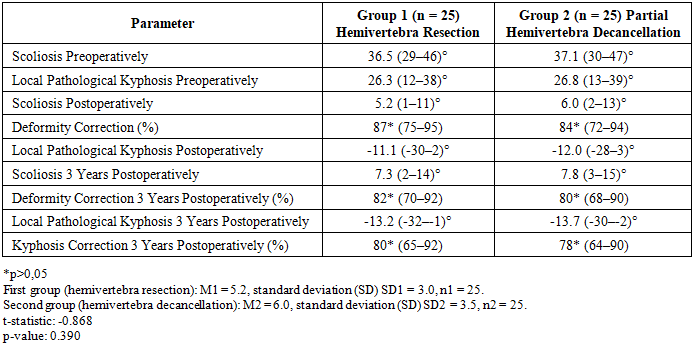
- The conducted study showed that surgical treatment of congenital scoliosis of the lumbar spine using both resection and partial decancellation of the hemivertebrae results in comparable deformity correction outcomes. Three years after surgery, both groups exhibited stability in the achieved results without significant progression of the scoliotic or kyphotic components of the deformity. Postoperative data analysis revealed that with hemivertebra resection, a high degree of correction was achieved in both the frontal and sagittal planes by completely eliminating the pathological growth center. However, this method was associated with greater surgical trauma, increased operation time, and more pronounced intraoperative blood loss. In the group of patients who underwent partial decancellation of the hemivertebra, significant correction of the deformity was also achieved, similar to the resection group results. However, this method showed less blood loss, which contributed to a reduced risk of intraoperative complications, as well as a decreased need for massive infusion therapy and blood transfusions in the postoperative period.Thus, considering the comparable results of scoliosis correction with both techniques, but with less intraoperative trauma and blood loss in decancellation, this method can be recommended as an alternative option for surgical treatment of congenital scoliosis in children, particularly in patients with a high risk of complications.
4. Conclusions
- The study demonstrated that the surgical treatment of congenital scoliosis of the lumbar spine using both resection and partial decancellation of the hemivertebra results in nearly identical deformity correction outcomes. Three years after surgery, both groups showed stability in the achieved results, with no significant progression of the scoliotic or kyphotic components of the deformity. Postoperative data analysis revealed that the partial decancellation of the hemivertebra achieved a level of correction comparable to that of resection, both in the frontal and sagittal planes. In addition, decancellation led to less intraoperative blood loss and a reduced risk of complications, contributing to a shorter operative time and less need for extensive infusion therapy and blood transfusions in the postoperative period.Therefore, considering that the results of scoliosis correction with both methods are nearly identical, and with the decancellation technique showing reduced intraoperative trauma and blood loss, we conclude that partial decancellation of the hemivertebra is just as effective as resection and can be recommended as a viable alternative for the surgical treatment of congenital scoliosis, particularly for patients at higher risk of complications.