-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(1): 243-246
doi:10.5923/j.ajmms.20261601.54
Received: Jan. 3, 2026; Accepted: Jan. 20, 2026; Published: Jan. 22, 2026

Combined Surgical Interventions in the Treatment of Ventral Hernias in Patients with Morbid Obesity
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAskarov P. A., Bazarov B. B., Kurbanyiazov Z. B.
Samarkand State Medical University, Samarkand, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The results of surgical treatment of 156 patients with morbid obesity and ventral hernias were analyzed. The comparison group included 54 patients who underwent isolated hernioalloplasty. The study group consisted of 102 patients who underwent simultaneous surgeries, including hernioalloplasty, abdominoplasty, and correction of concomitant surgical pathology of the abdominal and pelvic organs. Intraoperative parameters, complication rate, long-term results, and quality of life were assessed using the SF-36 questionnaire. All patients in the study group were found to have concomitant surgical pathology, most commonly abdominal adhesive disease, cholelithiasis, and pelvic pathology. The use of a combined surgical approach reduced the incidence of wound complications (13.7% versus 35.2% in the comparison group), decreased the risk of ventral hernia recurrence (3.1% versus 16.3%), and shortened the duration of hospitalization. According to the SF-36, a significant improvement in the physical, psychoemotional, and social components of quality of life was noted. Combined hernioalloplasty with abdominoplasty and simultaneous correction of concomitant pathology is a pathogenetically justified and clinically effective method for treating ventral hernias in patients with morbid obesity.
Keywords: Ventral hernias, Morbid obesity, Simultaneous operations, Abdominoplasty, Hernioalloplasty
Cite this paper: Askarov P. A., Bazarov B. B., Kurbanyiazov Z. B., Combined Surgical Interventions in the Treatment of Ventral Hernias in Patients with Morbid Obesity, American Journal of Medicine and Medical Sciences, Vol. 16 No. 1, 2026, pp. 243-246. doi: 10.5923/j.ajmms.20261601.54.
1. Introduction
- Ventral hernias in patients with morbid obesity represent one of the most complex and challenging issues in modern abdominal surgery. This is due to a combination of pronounced [1] anatomical and functional changes in the anterior abdominal wall, including abdominoptosis, a massive skin and fat apron, persistently elevated intra-abdominal pressure, and a high incidence of concomitant surgical pathology of the abdominal and pelvic organs. In this patient population, ventral hernia is typically not an isolated condition but develops in the context of systemic disorders associated with obesity, significantly complicating the choice of optimal surgical approach.The use of traditional isolated hernioalloplasty methods in patients with morbid obesity is associated with a high incidence of wound and extra-abdominal complications, technical difficulties during surgery, and recurrence of ventral hernias in the late postoperative period. Persistent severe abdominoptosis and massive subcutaneous fat after hernioplasty lead to disruption of the biomechanics of the anterior abdominal wall, uneven distribution of loads on the mesh implant fixation area, and deterioration of the conditions for reparative processes. The presence of concomitant surgical pathology further increases the scope of the intervention and the risk of adverse outcomes [2].In recent years, increasing attention has been paid to simultaneous surgical interventions aimed at the simultaneous correction of several pathological conditions in this category of patients. This approach is seen as an opportunity not only to eliminate the hernia defect but also to address key pathogenetic factors that determine the development of complications and recurrence. In particular, the combination of hernialloplasty and abdominoplasty allows for the restoration of the anatomical and functional integrity of the anterior abdominal wall and the reduction of pathological loads on the reconstruction area. However, the safety, feasibility, and clinical efficacy of combined hernioalloplasty and abdominoplasty in patients with morbid obesity remain controversial. The impact of these simultaneous procedures on the incidence of postoperative complications, long-term treatment outcomes, and patient quality of life, as well as the patient selection criteria for this [3] approach, remain insufficiently studied. This underscores the relevance of further research aimed at substantiating optimal surgical approaches for patients with ventral hernias and morbid obesity.The aim of this study was to evaluate the efficacy and safety of combined surgical approaches in patients with ventral hernias and morbid obesity.
2. Material and Methods
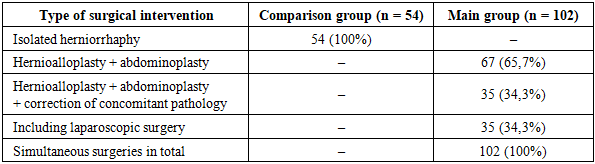
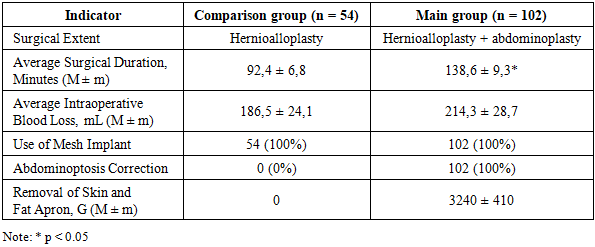
- The study included 156 patients with morbid obesity and ventral hernias, who were treated in the surgical department of a multidisciplinary hospital. Patients were selected based on clinical and instrumental examinations, taking into account the degree of obesity, the size and location of the hernia defect, and the presence of concomitant surgical pathology of the abdominal cavity and pelvis. All patients underwent elective surgery after standard preoperative preparation.Depending on the chosen surgical approach, patients were divided into two comparable groups. The comparison group (n=54) included patients who underwent isolated hernialloplasty using tension-free methods of anterior abdominal wall reconstruction. The main group consisted of 102 patients who underwent a combined surgical approach, including hernioalloplasty, abdominoplasty and simultaneous correction of concomitant surgical pathology of the abdominal and pelvic organs.
|
|
|
3. Results
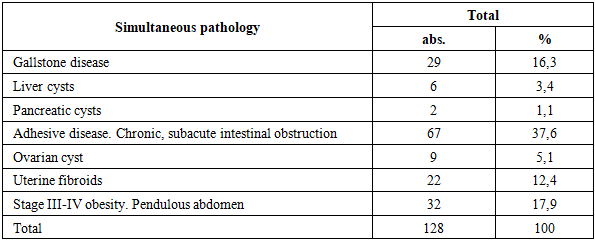
- All patients in the study group had concomitant surgical pathologies requiring immediate correction, confirming the high prevalence of comorbidities in patients with morbid obesity and ventral hernias. The most common comorbidities included abdominal adhesive disease (37.6%), grades III–IV obesity with a prominent pendulous abdomen (17.9%), cholelithiasis (16.3%), and pelvic pathology in women. The presence of these conditions significantly impacted the extent and sequence of surgical intervention and required individualized planning of a simultaneous surgical approach.The use of a combined surgical approach was associated with a significant reduction in the incidence of wound complications compared to the comparison group. In the study group, a decrease in the incidence of seromas, infiltrates, and suppuration of the postoperative wound was noted. This was associated with the removal of massive subcutaneous fat, improved tissue healing, and reduced pathological stress on the reconstructed anterior abdominal wall. The recurrence rate of ventral hernias in the study group was 3.1%, compared to 16.3% in the comparison group, indicating greater stability of anatomical and functional results with the simultaneous approach.Furthermore, patients in the study group demonstrated a shorter hospital stay and earlier postoperative mobilization. This, in turn, reduced the risk of extra-abdominal complications and accelerated rehabilitation. The more favorable postoperative course confirms the safety and clinical feasibility of expanding the scope of the intervention through simultaneous correction of comorbidities. An analysis of quality-of-life indicators using the SF-36 questionnaire revealed a significant improvement in physical functioning, a reduction in pain severity, and increased social activity in patients in the study group. Improved psychoemotional state and social adaptation indicators reflected the restoration of functional integrity of the anterior abdominal wall and increased patient satisfaction with the surgical results. Taken together, the obtained data confirm that combined surgical approaches not only provide better clinical outcomes but also facilitate comprehensive functional and social rehabilitation in patients with ventral hernias and morbid obesity.
4. Discussion
- The obtained results indicate that isolated hernia alloplasty in patients with morbid obesity does not eliminate the key pathogenetic factors of hernia formation and recurrence. Persistent severe abdominoptosis, a massive skin-fat apron, increased intra-abdominal pressure, and concomitant surgical pathology lead to disruption of the biomechanics of the anterior abdominal wall, uneven load distribution in the mesh implant fixation area, and a deterioration in the conditions for strong scar formation [6]. This explains the higher rate of wound complications and ventral hernia recurrence with isolated hernia alloplasty in this category of patients.Incorporating abdominoplasty and simultaneous correction of concomitant surgical pathology allows for addressing the key pathogenetic factors of the disease. Removal of the skin and fat apron and correction of abdominoptosis help reduce static and dynamic loads on the reconstructed anterior abdominal wall, restore its anatomical and functional integrity, and improve biomechanical conditions in the hernioplasty area. Simultaneous treatment of concomitant abdominal and pelvic pathologies reduces the cumulative impact of factors contributing to intra-abdominal hypertension and chronic inflammation, which positively impacts the postoperative course.Of particular significance is the fact that the use of a simultaneous approach was not associated with an increased incidence of intra- or postoperative complications, despite the increased surgical scope. On the contrary, the data obtained demonstrate a more favorable [8] early postoperative course, a reduced incidence of wound complications, and a significant reduction in the risk of ventral hernia recurrence at long-term follow-up. This confirms that increasing the surgical scope through functionally justified stages does not equate to an increased surgical risk [14].
5. Conclusions
- Combined hernioalloplasty with abdominoplasty and simultaneous correction of concomitant surgical pathology is an effective and safe treatment method for patients with ventral hernias and morbid obesity. This approach reduces the incidence of complications and recurrence, improves quality of life, and can be recommended for widespread implementation in clinical practice.