-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(1): 229-233
doi:10.5923/j.ajmms.20261601.50
Received: Dec. 27, 2025; Accepted: Jan. 19, 2026; Published: Jan. 22, 2026

The Results of Treatment of Acute Appendicitis on the Background of Liver Cirrhosis are Presented
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLUrokov Sh. T., Abidov U. O., Khudaybergenov Sh. O.
Bukhara State Medical Institute named after Abu Ali ibn Sina, Bukhara, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

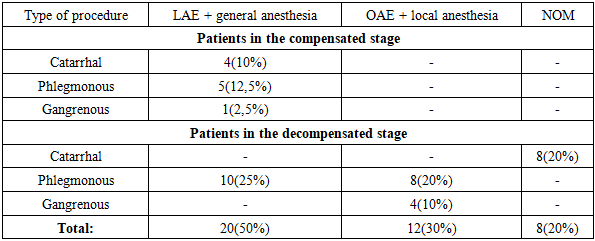
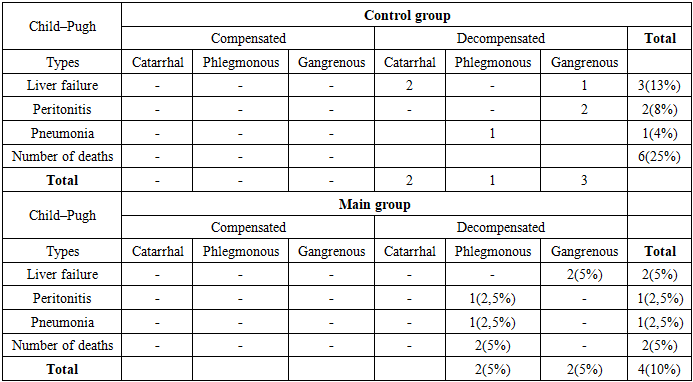
The development of acute appendicitis in patients with liver cirrhosis presents significant clinical and diagnostic challenges. A retrospective analysis examined complications and mortality in 24 patients with LC. In the postoperative period, wound suppuration (29%), bleeding (8.3%), sepsis and pneumonia (8.3%), peritonitis (8.3%), and mortality in 25% of cases were observed. These complications were mainly recorded in patients with decompensated LC. In the main (prospective) group, 40 patients were examined and treated. The treatment strategy was determined based on extended diagnostics (MRI, C-reactive protein, and biochemical tests). In cases of catarrhal appendicitis (20%), conservative treatment (NOM) was successfully applied. In the compensated stage, laparoscopic appendectomy (LAE) was found to be the optimal method, whereas in the decompensated stage, open appendectomy (OAE) under local anesthesia was recommended. As a result, the complication and mortality rate decreased from 25% in the control group to 10% in the main group. This is explained by the effective integration of preventive measures into the treatment strategy. The diagnosis and treatment of AA in patients with LC require the use of modern diagnostic tools, minimally invasive approaches, and stratification of treatment tactics according to the patient’s functional condition.
Keywords: Liver cirrhosis, Acute appendicitis, Laparoscopic appendectomy, Open appendectomy, NOM, Surgical methods
Cite this paper: Urokov Sh. T., Abidov U. O., Khudaybergenov Sh. O., The Results of Treatment of Acute Appendicitis on the Background of Liver Cirrhosis are Presented, American Journal of Medicine and Medical Sciences, Vol. 16 No. 1, 2026, pp. 229-233. doi: 10.5923/j.ajmms.20261601.50.
1. Introduction
- The development of acute appendicitis against the background of liver cirrhosis causes difficulties in diagnosing and treating the disease in patients. In patients with liver cirrhosis, due to disturbances in portal circulation and impairment of hepatic metabolic functions, it is natural that a number of specific features are observed in the clinical presentation of appendicitis.Given the increasing prevalence of liver cirrhosis worldwide, the aim of this systematic review was to determine the risk of perioperative mortality after appendectomy in such patients [5,6,7].According to data from various authors, the mortality rate in acute appendicitis ranges from 0.14% to 0.5%, while among elderly and senile patients it reaches 4.6%. It should be noted that among patients hospitalized within the first 6 hours after the onset of the disease, the mortality rate is only 0.02%; in the period from 6 to 24 hours it is 0.09%, and after 24 hours this figure increases to 1%. These numbers may not seem particularly high; however, considering the annual number of operations performed for acute appendicitis (1–1.5 million), the absolute number of deaths is quite substantial—approximately 4,000 per year [1,2,4,5,9].According to Adiamah A. and Rashid A. (2023), the risk of mortality after appendectomy in patients with liver cirrhosis is higher than in the general population. This is associated with an increased risk of perioperative complications, including bleeding, infections, and hepatic decompensation [2].Appendectomy is the most common emergency abdominal surgical procedure in the United Kingdom, with more than 42,000 such operations performed annually. In the general population, this procedure is considered safe, with a 30-day mortality rate of only 0.244%. However, this indicator increases in patients over 60 years of age, as well as in those diagnosed with perforated appendicitis [2,3,5,11].Nevertheless, there is a relative lack of comprehensive studies dedicated to the management of acute appendicitis in the setting of liver cirrhosis. Therefore, conducting a detailed investigation is of significant importance to fill this gap in medical knowledge. From a theoretical perspective, the course of acute appendicitis against the background of liver cirrhosis may lead to serious complications. In our study, we aimed to investigate the outcomes of acute appendicitis in patients with liver cirrhosis, as well as to analyze their mortality rates and associated comorbidities [8,10,11].Aim of the study. To evaluate the outcomes of diagnostic and treatment methods in cases where liver cirrhosis is associated with acute appendicitis, and to develop effective management approaches.
2. Materials and Methods
- The study materials included a retrospective analysis of 24 (0.8%) medical records of patients with acute appendicitis treated in the emergency surgery departments of the Bukhara branch of the Republican Specialized Scientific and Practical Medical Center during 2017–2020, as well as a prospective analysis of the outcomes of the proposed diagnostic and therapeutic strategy in 40 (1.4%) patients examined and treated for acute appendicitis during 2021–2024.In the control group of patients, treatment included antibacterial therapy (cephalosporins, fluoroquinolones), detoxification and infusion therapy. Surgery was performed as OAE via the Volkovich–Dyakonov incision. Anesthesia was general anesthesia. The outcomes of surgical treatment were analyzed, including wound suppuration, infectious complications, progression of hepatic failure, length of hospital stay, in-hospital mortality, 30-day readmission, and other parameters.In addition to routine clinical examinations, patients in the main group with liver cirrhosis and suspected acute appendicitis underwent extended instrumental diagnostic methods (MRI) to assess the condition of acute appendicitis and to determine the optimal treatment strategy.Besides standard complete blood count tests, patients in the main group underwent liver biochemical analyses (bilirubin, ALT, AST, total protein, creatinine, HBsAg, HBeAg, anti-HBe, anti-HBc markers), international normalized ratio (INR), and C-reactive protein blood tests.The treatment strategy was determined based on the results of instrumental and laboratory investigations, taking into account the degree of hepatic functional impairment according to the Child–Pugh classification. In addition to standard therapy, the treatment regimen included ceftriaxone, Hepa-Merz, glutathione, albumin, concentrated glucose solutions, and vicasol.In the main group of patients, surgeries were performed as LAE using ultrasonic dissectors (anesthesia: general anesthesia) as well as OAE via the Volkovich–Dyakonov incision (anesthesia: local or epidural anesthesia).The distribution of patients by sex in the control and main groups is presented (Table 1). Women accounted for 14 cases (58.3%) in Group I and 23 cases (57.5%) in Group II, with a total of 37 women (58.8%). Men were recorded in 10 cases (41.7%) in the control group and 17 cases (42.5%) in the main group.
|
|
|
3. Discussion of Results
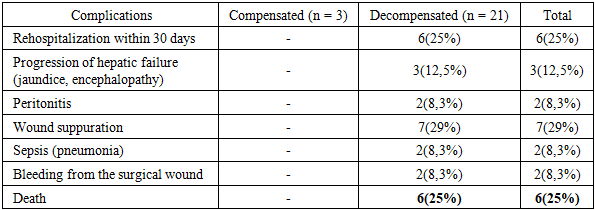
- The development of acute appendicitis in patients with liver cirrhosis is of considerable clinical and diagnostic significance, as the coexistence of these two conditions poses a number of challenges for clinicians. This is evidenced by the complications and mortality rates observed in the control group (based on retrospective analysis). Cirrhosis-associated immunosuppression, hypoalbuminemia, and coagulopathy place these patients in a high-risk category and lead to a range of life-threatening complications.A retrospective analysis of medical records of 40 patients operated on for acute appendicitis in the setting of liver cirrhosis revealed a number of complications and mortality outcomes. Due to complications, 6 patients (25%) were rehospitalized within 30 days after surgery with various postoperative complications. Although the surgical procedure itself was not technically difficult, postoperative cirrhosis-related complications led to death in 6 patients (25%). A particularly important and challenging aspect of the clinical analysis was that among the deceased patients, cases of the catarrhal form of appendicitis were also observed.Therefore, in the main group of patients, the focus was placed on assessing the degree of inflammation of the vermiform appendix in the preoperative period using MRI and C-reactive protein as a laboratory diagnostic marker, as well as on determining the feasibility of treating patients with decompensated liver cirrhosis using NOM. In addition, efforts were directed toward selecting optimal surgical techniques and anesthesia methods, avoiding abdominal cavity drainage at the end of surgery, and preventing cirrhosis-related complications in the postoperative period.
4. Conclusions
- 1. Analyses of the control group demonstrated that liver cirrhosis and its complications have a significant impact on the postoperative period. Among these patients, complications such as wound suppuration, bleeding, sepsis, peritonitis, and hepatic failure were observed. In addition, rehospitalization and mortality rates were high.2. In the compensated stage of liver cirrhosis, due to the relatively stable general condition, the use of minimally invasive laparoscopic appendectomy is appropriate. In the decompensated stage, if destructive changes of the vermiform appendix are present, open appendectomy under local anesthesia is advisable.3. Based on MRI findings, in non-destructive cases (catarrhal form) where surgical intervention carries a high risk, the use of antibacterial (conservative non-operative management, NOM) treatment improves clinical outcomes.4. In conclusion, in emergency medical practice it is essential to apply clinical assessment tools more broadly and purposefully to stratify patients with suspected AA. For patients with a low probability of acute appendicitis, observation is the most effective strategy. In patients at intermediate risk with an unclear clinical presentation, we recommend more detailed preoperative imaging studies. If imaging does not reveal pathology, additional examinations or continued observation are appropriate, and unnecessary haste in proceeding to surgery should be avoided.