-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(1): 208-211
doi:10.5923/j.ajmms.20261601.47
Received: Dec. 22, 2025; Accepted: Jan. 16, 2026; Published: Jan. 22, 2026

Analysis of the Role of Family and Migration Influence in the Spread of Scabies
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLA. T. Togaev1, E. Kh. Eshboev2
1Termez Branch of Tashkent State Medical University, Termiz, Uzbekistan
2Republican Specialized Scientific and Practical Medical Center of Dermatovenerology and Cosmetology, Tashkent, Uzbekistan
Correspondence to: A. T. Togaev, Termez Branch of Tashkent State Medical University, Termiz, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Our conducted research has shown that the family factor plays a key role in the spread of scabies in the Surkhandarya region. It was found that in 54.7% of cases (254 individuals), the disease was contracted from family members. In addition, internal and external migration is also an important factor in the spread of the disease. A high prevalence of the disease among labor migrants has been recorded.
Keywords: Scabies, Epidemiology, Clinical forms, Family hearths
Cite this paper: A. T. Togaev, E. Kh. Eshboev, Analysis of the Role of Family and Migration Influence in the Spread of Scabies, American Journal of Medicine and Medical Sciences, Vol. 16 No. 1, 2026, pp. 208-211. doi: 10.5923/j.ajmms.20261601.47.
1. Introduction
- Scabies is a highly contagious infectious disease caused by microscopic mites - *Sarcoptes scabiei var hominis*. The female mite burrows into the epidermis, parasitizes, and lays numerous eggs. Subsequently, the host organism mounts an immune response to this condition, resulting in skin rashes and intense itching [1,2,3]. It was only in 2017 that the WHO classified scabies as one of the neglected tropical diseases. Notably, more than 200-250 million people worldwide are affected by scabies annually [4,5,6].The spread of the scabies pathogen (mite) among humans has a focal nature and is associated with their lifestyle and behavior. The source of scabies is considered to be an infected person. Within a group of people (in conditions where the pathogen can spread), a single patient with scabies can create a disease focus. Typically, a focus with one patient is referred to as a potential focus, while a focus with two or more patients is called an active (transmissible) focus [7,8].There is a close relationship between the epidemiological process and the population structure of the pathogen. In this case, mites in their reproductive stage multiply on the patient's skin (elementary population). The interaction between the macroorganism and the pathogen manifests itself in the clinical presentation of the disease.At the second population level, the etiological factor increases in a group of people (patients). When new individuals are infected, the proportion of mites in their reproductive stage also increases. At the third level, reproduction spreads among the population in villages, districts, cities, and regions. At this level, the significance of the biological factor in the increase of the disease diminishes, while social and household-communal factors come to the forefront.Considering that people work in organized collectives and live in families with many members, as well as interact with each other, the foci of scabies can occur within families and communities.The increase in the duration of the disease in a family focus is directly proportional to the spread of scabies. The disease is initially brought into the family by one of its members; sometimes, it can enter from outside when relatives or acquaintances stay overnight for several days. Young adolescent boys and girls often contract the disease when they share a room with friends or companions.The aim of the research is to conduct a comparative assessment of familial and non-familial transmission among individuals diagnosed with scabies in Surkhandarya region, and to study the impact of internal and external migration on this transmission.The research objects included epidemic and outpatient records of 5,050 scabies patients identified during 2010-2024 in the Surkhandarya region, medical histories of 464 patients undergoing inpatient treatment, a list of patients under outpatient and dispensary observation, examination documents of their household contacts, as well as annual reports at the district, regional, and national levels.The subjects of the study were 464 patients in our research, as well as their household contacts, and pathological materials obtained from skin scrapings for microscopic examination (scabies mites).
2. Research Methods
- In the scientific research process, epidemiological, clinical (retrospective epidemiological analysis), bacterioscopic studies, and statistical (Pearson's chi-square (χ2) coefficient, variation analysis, and Fisher's method) research methods were used.We aimed to study the influence of family clusters, internal and external migration on the spread of scabies. When we examined 464 patients under our observation for the presence of familial clusters, it was determined that 254 (54.7%) patients had contracted the disease from one of their family members (Figure 1).Mites are active at night and transmission occurs more frequently during nighttime.
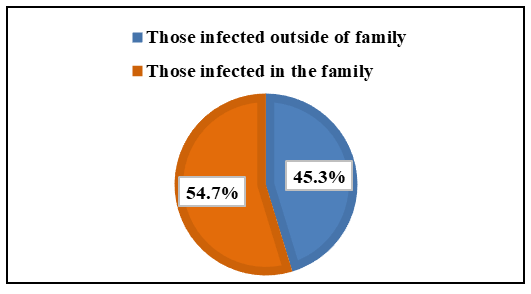 | Figure 1. Distribution of family and non-family transmission among 464 patients diagnosed and treated for scabies |
 | Figure 2. Clinical presentation of scabies on the skin of a 3-month-old baby |
 | Figure 3. Appearance of rashes on the leg skin of an 8-month-old child with scabies |
 | Figure 4. Appearance of rash on palms of newborn with scabies |
 | Figure 5. Appearance of skin rash on abdomen of newborn with scabies |
3. Results
- Scabies primarily spreads through family clusters (54.7% of cases). Infants aged 1-2 years often contract it directly from their mothers, and in many cases, the condition is misdiagnosed.Cases of sexual transmission were observed, particularly among young men (28.2% of cases).A high prevalence of the disease was found among labor migrants (33.4% of cases).Informal labor activities and hired workers are also significant factors in the spread of the disease.
4. Conclusions
- Thus, the role of family factors, as well as internal and external migration, in the spread of scabies in certain areas is convincingly high. Indeed, it is necessary to take this information into account when developing treatment and preventive measures against scabies.Based on these observations and considerations, we offer the following recommendations: • It is necessary to regulate the registration of cases and the monitoring of their contacts; • Continuously publish manuals and methodological guidelines that fully cover the epidemiology, treatment, and current advanced prevention of the disease; • Implement preventive chemotherapy and the widespread use of medicinal substances in practice; • Systematically organize training to improve the qualifications of all staff involved in or wishing to engage in laboratory diagnosis of scabies mites; • Continuously carry out pre-planned sanitary-educational and preventive activities among the population.Raise awareness about scabies prevention and increase the level of public medical knowledge in this area through television, radio, newspapers, and specialized social media platforms.