-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(1): 197-199
doi:10.5923/j.ajmms.20261601.44
Received: Dec. 29, 2025; Accepted: Jan. 22, 2026; Published: Jan. 22, 2026

Clinical and Pathogenetic Features of Lipid Metabolism Disorders and the Development of Obesity in COVID-19 Patients
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKhairullaeva G. S.
Bukhara State Medical Institute, Bukhara, Uzbekistan
Correspondence to: Khairullaeva G. S., Bukhara State Medical Institute, Bukhara, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The analysis showed that in COVID-19 patients, lipid metabolism disorders and the severity of systemic inflammation progress as the degree of obesity increases. In patients with severe obesity, maximum levels of atherogenic lipids, inflammatory markers, and insulin resistance were identified, which are accompanied by adipokine imbalance. These changes contribute to the worsening of COVID-19 and determine the need for early metabolic correction in this category of patients.
Keywords: COVID-19, Obesity, Lipid metabolism, Dyslipidemia, Insulin resistance, Adipokines, Leptin, Adiponektin, Systemic inflammation, IL-6, CRP
Cite this paper: Khairullaeva G. S., Clinical and Pathogenetic Features of Lipid Metabolism Disorders and the Development of Obesity in COVID-19 Patients, American Journal of Medicine and Medical Sciences, Vol. 16 No. 1, 2026, pp. 197-199. doi: 10.5923/j.ajmms.20261601.44.
1. Introduction
- The COVID-19 pandemic coincided with global obesity growth, forming a combination of two major epidemics. Patients with excess body weight significantly more often require hospitalization and have a more severe course of COVID-19, which is associated with metabolic disorders, chronic inflammation, and atherogenic dyslipidemia [1,2,3,4]. Obesity is considered an independent risk factor for respiratory failure, thrombosis, and mortality, while the combination of obesity with dyslipidemia and insulin resistance forms an unfavorable metabolic phenotype in the patient [2,3,4,5,6].The pathogenesis of COVID-19 in obesity is associated with lipid metabolism disorders, a decrease in HDL cholesterol and LDL levels, an increase in triglycerides, and the active production of pro-inflammatory cytokines [7,8,9,10]. SARS-CoV-2 is capable of infecting adipocytes and macrophages of adipose tissue, intensifying local and systemic inflammation, insulin resistance, and metabolic dysfunction [11,12,13]. These processes exacerbate the course of COVID-19 and explain the high frequency of complications in patients with obesity.Correction of lipid metabolism disorders is considered an important area of treatment for COVID-19 patients. The effectiveness of statins, omega-3 LDLs, fibrates, and non-drug interventions (diet, weight reduction) has been confirmed by clinical data showing a decrease in the frequency of complications and improvement in outcomes [9,14,15,16]. However, optimal management strategies for patients with obesity and COVID-19 require further study, which determines the relevance of this study.The purpose of the study is to identify the clinical and pathogenetic features of lipid metabolism disorders and the mechanisms of obesity development in COVID-19 patients, as well as to evaluate the effectiveness of various methods for correcting dyslipidemia and metabolic dysfunction in the acute and post-infectious course of the disease.
2. Materials and Methods of Research
- The study was conducted under multicenter observation and included 168 patients who had COVID-19 of varying severity and had signs of lipid metabolism disorders. The selection was carried out on the basis of the infectious diseases hospital and the consultative and diagnostic center. The age of the examined varied from 28 to 72 years (average age 49.6 ± 12.1 years); among them were 92 men (54.8%) and 76 women (45.2%). Inclusion criteria included laboratory-confirmed SARS-CoV-2 (PCR), presence of dyslipidemia or obesity (MI≥ 30 kg/m2), and consent to participate in the study.To analyze the characteristics of lipid metabolism, patients were divided into three groups. Group I (n=54) included patients with normal body weight and moderate dyslipidemia in COVID-19; Group II (n=62) - patients with obesity of I-II degree, who had COVID-19 in moderate form; Group III (n=52) consisted of patients with obesity of the III degree and pronounced lipid profile disorders who had a severe form of the disease. This distribution made it possible to assess the influence of the degree of obesity and the severity of metabolic disorders on the clinical course of COVID-19.
3. Research Results
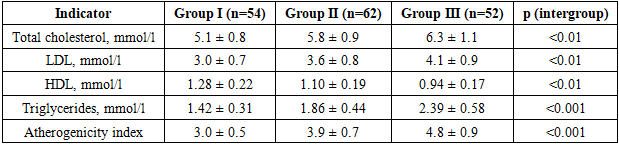
- Analysis of 168 COVID-19 patients showed significant differences in lipid metabolism and metabolic status between the groups. The progression of obesity was accompanied by an increase in the frequency of moderate to severe COVID-19, as well as a deterioration in laboratory inflammatory parameters and lipid profile (Table 1).
|
|
4. Output
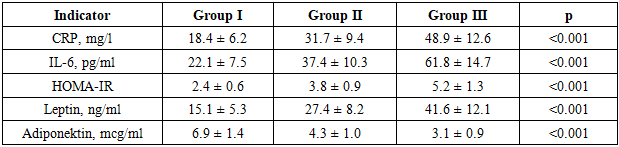
- As a result of the conducted research, it was established that the increase in the degree of obesity in COVID-19 patients is accompanied by a significant increase in lipid metabolism disorders, a pronounced increase in pro-inflammatory markers (CRP, IL-6), progression of insulin resistance, and adipokine imbalance, which forms an unfavorable metabolic and inflammatory background that worsens the course of the disease. The most pronounced deviations were found in patients with severe obesity, who exhibited maximum values of atherogenic lipids, hyperleptinemia, and minimal levels of adiponektin. The obtained results confirm the key role of obesity as a pathogenetic factor in the complicated course of COVID-19 and justify the need for early diagnosis and active correction of metabolic disorders in this category of patients.