-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(1): 187-190
doi:10.5923/j.ajmms.20261601.42
Received: Dec. 22, 2025; Accepted: Jan. 15, 2026; Published: Jan. 20, 2026

The Role of Morphological Changes in the Fetus and Placenta in Forensic Medical Diagnosis of Antenatal Fetal Death
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLNorova Kamola Malikovna1, Elieva Mehriniso Fakhriddinovna2
1Independent Researcher, Tashkent State Medical University, Tashkent, Uzbekistan
2Tashkent State Medical University, Tashkent, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

A total of 54 cases of antenatal fetal death referred for forensic medical examination between 2021 and 2024 were analyzed. The study was conducted at the Republican Scientific and Practical Center of Forensic Medical Expertise. The study included cases of intrauterine fetal death occurring before the onset of labor, as confirmed by clinical data, obstetric documentation, and morphological findings. The gestational age of the fetuses ranged from 22 to 40 weeks. Histological sections were stained with hematoxylin and eosin. Morphological assessment focused on signs of hypoxia, ischemia, circulatory disturbances, inflammatory changes, and dystrophic processes. The results demonstrated that, in the majority of antenatal fetal death cases, a complex of pathological changes in the placenta and fetal organs was identified, reflecting chronic intrauterine distress.
Keywords: Antenatal fetal death, Fetus, Placenta, Intrauterine death
Cite this paper: Norova Kamola Malikovna, Elieva Mehriniso Fakhriddinovna, The Role of Morphological Changes in the Fetus and Placenta in Forensic Medical Diagnosis of Antenatal Fetal Death, American Journal of Medicine and Medical Sciences, Vol. 16 No. 1, 2026, pp. 187-190. doi: 10.5923/j.ajmms.20261601.42.
1. Introduction
- Antenatal fetal death remains one of the leading public health and obstetric challenges worldwide, despite significant advances in prenatal diagnostics and perinatal care. According to national fetal mortality reports, the rate of intrauterine fetal death remains substantial and demonstrates only a slow decline in many developed countries, emphasizing the need for further investigation into the causes and mechanisms of fetal demise [1,2]. In forensic medical practice, postmortem examination of the fetus, and particularly morphological investigation of the placenta combined with fetal autopsy, plays a crucial role in establishing the cause of antenatal fetal death. Numerous studies indicate that without systematic postmortem examination, a significant proportion of cases remain unexplained, hindering the development of preventive strategies and objective legal assessment of fetal death [3,4,5]. Classification systems for perinatal mortality causes, such as CODAC, RECoDe, and others, demonstrate considerable variability depending on the selected criteria and hierarchical structure of contributing factors. This variability complicates data comparability and necessitates strict methodological standardization by forensic medical experts when documenting the thanatogenesis of antenatal fetal death [6,7,8]. Consequently, the development and implementation of standardized forensic diagnostic algorithms and reporting systems for antenatal fetal death remain a pressing issue. Pathomorphological studies indicate the leading role of placental pathology-including chronic placental insufficiency, vascular disorders, and placental infarctions-as well as intrauterine infection and fetal growth restriction, as key pathogenetic factors of antenatal fetal death. However, even in large cohorts, a substantial proportion of cases lack a clearly established cause of death, highlighting the need for advanced morphological, immunohistochemical, and molecular genetic investigations within forensic medical practice [9,10,11,12,13,14,15,16,17].Thus, the scientific and practical significance of this study is determined by several factors: the need to improve diagnostic accuracy in establishing the causes of antenatal fetal death; standardization of forensic medical protocols, including fetal autopsy, placental examination, and molecular genetic methods; development of recommendations aimed at preventing recurrent fetal losses and improving the quality of perinatal care. The implementation of unified forensic algorithms and standardized criteria for assessing the thanatogenesis of antenatal fetal death will enhance clinicopathological verification of causes of death, improve statistical reliability, strengthen preventive measures, and reduce the proportion of unexplained cases in forensic medical examinations.The purpose: The aim of the present study was to investigate the role of morphological changes in the fetus and placenta in the forensic medical diagnosis of antenatal death, based on the analysis of 54 cases of antenatal fetal demise.
2. Materials and Methods
- He study material comprised 54 cases of antenatal fetal death referred for forensic medical examination during the period 2021–2024. The study was conducted at a specialized forensic medical institution. The inclusion criteria were cases of intrauterine fetal death occurring before the onset of labor, as confirmed by clinical data, obstetric records, and the results of morphological examination. The gestational age of the fetuses ranged from 22 to 40 weeks.Histological sections were stained with hematoxylin and eosin. Morphological evaluation focused on signs of hypoxia, ischemia, inflammatory changes, circulatory disturbances, and dystrophic processes. Statistical analysis was performed using descriptive analytical methods.
3. Results and Discussion
- Morphological examination demonstrated that, in the majority of cases of antenatal fetal death, a complex of pathological changes in the placenta and fetal organs was identified, reflecting chronic intrauterine hypoxia and distress. In all cases, a complete forensic medical examination was performed, including external and internal examination of the fetus, macroscopic assessment of the placenta, umbilical cord, and fetal membranes, as well as histological examination of fetal tissues, including the lungs, heart, liver, kidneys, and brain. Histological evaluation of the placenta included detailed assessment of the villous tree, intervillous space, and placental vessels.The morphological study revealed that in most cases of antenatal fetal death, pathological changes in both the placenta and fetal organs were consistent with chronic intrauterine compromise. In 41 cases (75.9%), signs of chronic placental insufficiency of varying severity were identified. These changes included placental infarctions of different ages, fibrinoid necrosis of chorionic villi, sclerosis and obliteration of villous vessels, and marked fibrin deposition in the intervillous space. In 19 cases (35.2%), features of maternal–placental vascular disorders were observed, including thrombosis of spiral arteries and evidence of impaired transformation of uterine vessels. Inflammatory placental changes, such as chorioamnionitis and villitis, were identified in 12 cases (22.2%), predominantly in cases of preterm fetal death (Table 1).
|
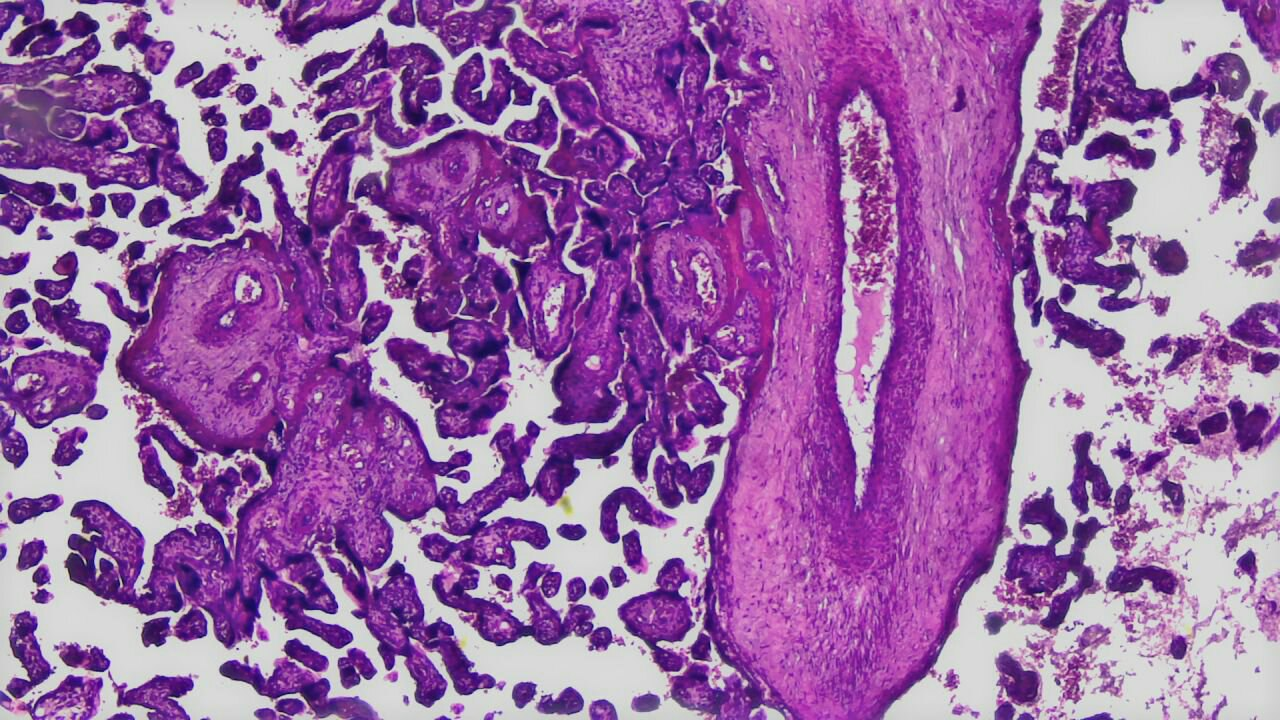 | Figure 1. The vascular lumen was sharply narrowed and partially obliterated. In the umbilical arteries, hypertrophy and vacuolization of smooth muscle cells of the media, vascular spasm, focal fibrosis. Stained with hematoxylin and eosin. Magnification 10×20 |
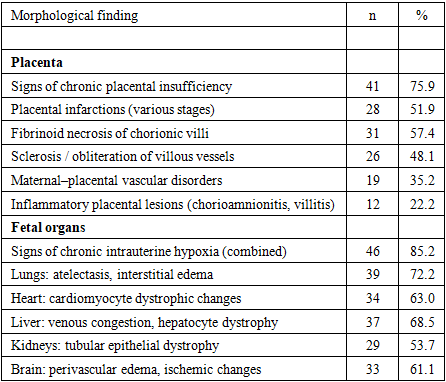
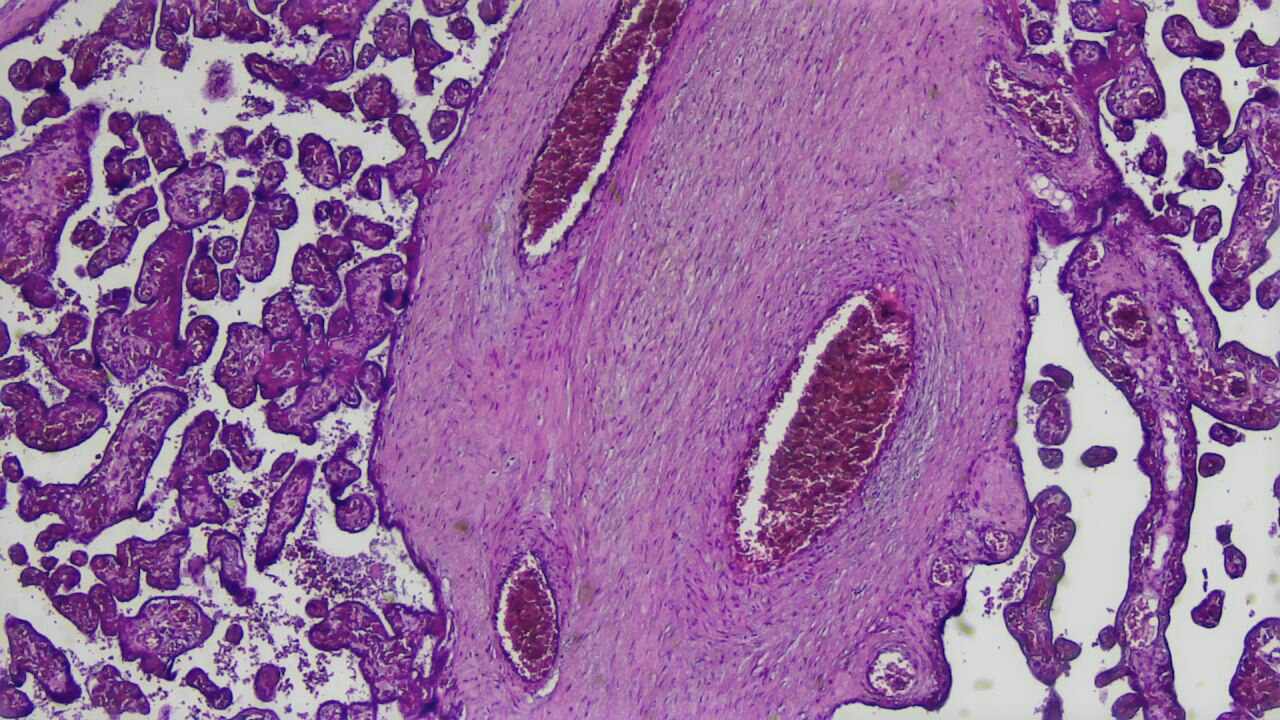
 | Figure 2. The examined histological specimen demonstrates fragments of chorionic villi of the placenta and a large umbilical cord vessel. Stained with hematoxylin and eosin. Magnification 10×20 |
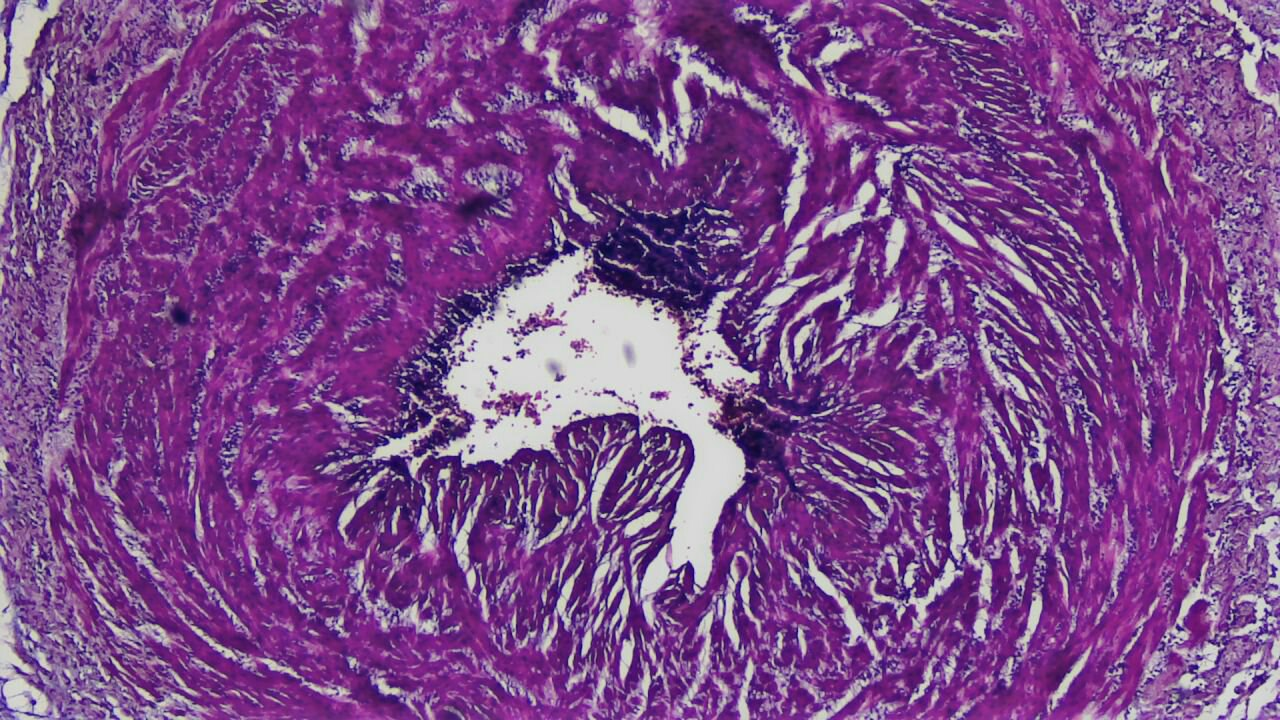
 | Figure 3. Demonstrates fragments of placental tissue with chorionic villi and areas of markedly fibrotic structures, corresponding to pathologically altered stem villi and vessels of fetal origin. Stained with hematoxylin and eosin. Magnification 10×20 |
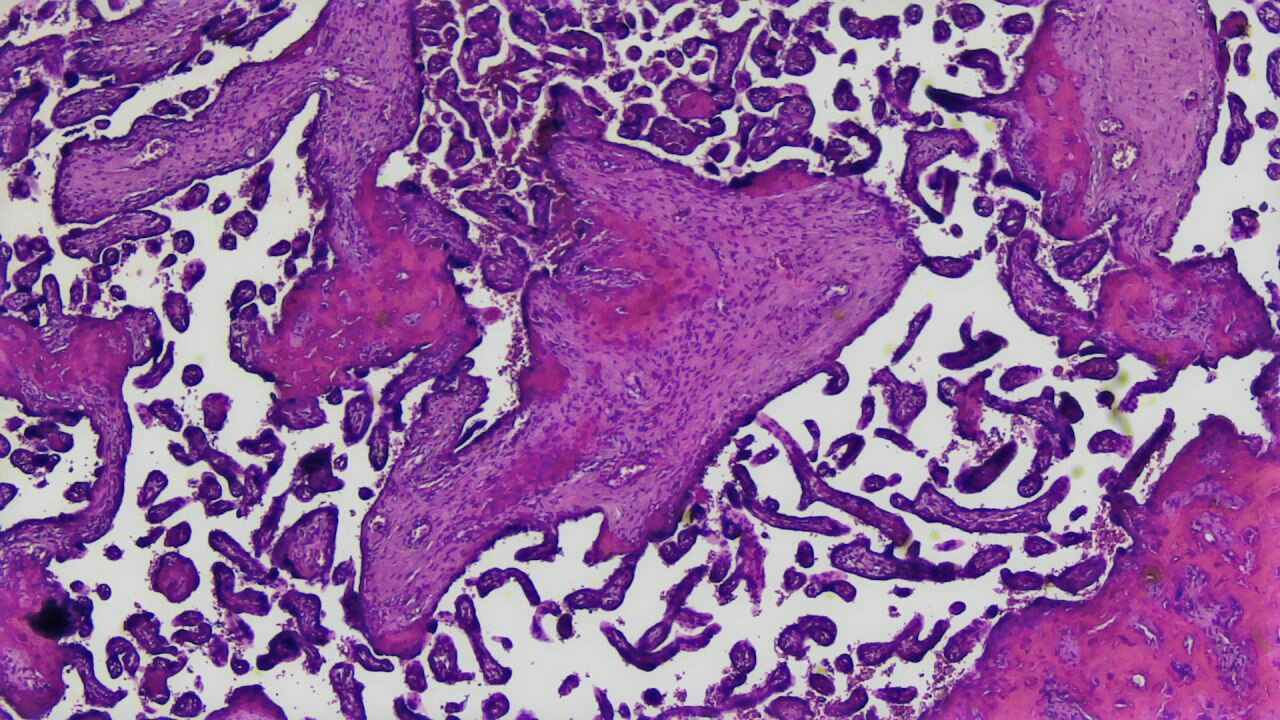
 | Figure 4. The villi are predominantly severely deformed and irregular in shape, with pronounced stromal sclerosis and hyalinosis. Stained with hematoxylin and eosin. Magnification 10×20 |
4. Conclusions
- The obtained results confirm the key role of morphological examination of the placenta and fetus in the forensic diagnosis of antenatal death. The placenta is the primary pathogenetic link, reflecting the duration and nature of fetal distress. Identified changes in the villous tree and placental vessels allow not only to establish the cause of death but also to estimate the time of death. Morphological changes in fetal organs, primarily signs of chronic hypoxia, complement the data from the placenta examination and provide a comprehensive picture of thanatogenesis. In forensic medicine, the differentiation of antenatal and intranatal deaths is of particular importance, which is only possible with a comprehensive morphological assessment. In the future, it is advisable to expand the morphological algorithm by using immunohistochemical markers of hypoxia, apoptosis, and inflammation, which will improve the accuracy of expert opinions.