-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(1): 180-182
doi:10.5923/j.ajmms.20261601.40
Received: Dec. 26, 2025; Accepted: Jan. 13, 2026; Published: Jan. 20, 2026

Modern Forensic Medical Criteria for Identifying Suicidal Risk in Women
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLElieva Mehriniso Fakhridinnovna
Tashkent State Medical University, Tashkent, Uzbekistan
Correspondence to: Elieva Mehriniso Fakhridinnovna, Tashkent State Medical University, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Suicidal behavior among women represents a complex medico-social and forensic medical problem that requires objective expert evaluation based on an integrated assessment of morphological, circumstantial, and clinical-anamnestic data. Key forensic medical criteria enabling differentiation of suicidal behavior from other forms of violent and non-violent death were identified. The most significant morphological and circumstantial features characteristic of female suicide cases were determined. A retrospective analysis of 165 autopsy cases of women submitted for forensic medical examination between 2021 and 2025 at the Republican Scientific and Practical Center of Forensic Medical Examination (Namangan Branch) was conducted. The results of the study demonstrate the feasibility and diagnostic value of applying systematized forensic medical criteria for the assessment of suicidal behavior in women.
Keywords: Suicidal behavior, Women, Forensic medical examination, Suicide risk, Medico-legal diagnostics, Forensic criteria
Cite this paper: Elieva Mehriniso Fakhridinnovna, Modern Forensic Medical Criteria for Identifying Suicidal Risk in Women, American Journal of Medicine and Medical Sciences, Vol. 16 No. 1, 2026, pp. 180-182. doi: 10.5923/j.ajmms.20261601.40.
1. Introduction
- Suicidal behavior among women remains a major public health issue with significant medico-social and legal consequences. Female suicide is influenced by a complex interaction of biological, psychological, hormonal, and social factors, including affective disorders, chronic stress, interpersonal conflicts, reproductive and endocrine disturbances, and socio-cultural expectations. These factors contribute to gender-specific patterns of suicidal behavior, which often differ from those observed in men [1,2,3].In forensic medical practice, the determination of suicide as the manner of death in women presents particular challenges. Female suicidal acts are frequently characterized by less violent methods, ambiguous injury patterns, and circumstances that may mimic accidental death. As a result, suicide in women is often underdiagnosed or misclassified, especially in cases lacking clear circumstantial evidence [4].Modern forensic diagnostics increasingly emphasizes the necessity of an integrated assessment that combines morphological findings, scene investigation data, toxicological results, and clinical-anamnestic information. However, the absence of standardized, gender-oriented forensic criteria limits the consistency and reproducibility of expert conclusions. Diagnostic uncertainty may lead to legal misinterpretation and negatively affect both judicial outcomes and suicide prevention strategies [5,6,7].In this context, the development of systematized forensic medical criteria for assessing suicidal behavior in women is of critical importance. Such criteria should account for gender-specific manifestations of suicide and provide a structured framework for expert analysis.ObjectiveTo develop and systematize forensic medical criteria for the assessment of suicidal behavior in women based on a comprehensive analysis of autopsy material and associated medico-legal data.
2. Materials and Methods
- A retrospective analysis was conducted on 165 autopsy cases of women who underwent forensic medical examination between 2021 and 2025 at the Republican Scientific and Practical Center of Forensic Medical Examination (Namangan branch). The study material included autopsy reports, histological findings, toxicological test results, investigative records, and available medical documentation. Cases were classified according to the manner of death and included completed suicides, attempted suicides with survival, and deaths from natural causes used as a comparative group. Morphological criteria were evaluated with particular attention to the nature, localization, multiplicity, and vitality of injuries. Circumstantial factors included scene investigation data, body position, evidence of struggle, and the presence of suicide-associated objects.Medico-biological indicators comprised toxicological findings and morphofunctional changes in vital organs. Clinical, anamnestic, and social factors were analyzed based on medical histories and investigative documentation. In a subgroup of women who survived suicide attempts, validated psychometric instruments were used to assess suicidal risk. Comparative and statistical analyses were applied to determine the diagnostic significance of the identified criteria.
3. Results and Discussion
- The analysis demonstrated that forensic assessment of suicidal behavior in women requires a multidimensional approach. Morphological findings alone were insufficient to establish suicide with high diagnostic certainty, particularly in cases with atypical injury patterns or minimal external trauma.In suicidal cases, characteristic injury features included method-consistent localization, limited defensive injuries, and clear signs of vitality. Circumstantial analysis revealed that scene characteristics such as the absence of struggle, body positioning, and contextual evidence played a crucial role in differentiating suicide from accidental or criminal death.Medico-biological indicators, including toxicological results and morphofunctional changes in vital organs, provided essential corroborative evidence. Toxicological analysis frequently revealed psychoactive substances, alcohol, or medications capable of influencing behavioral control and emotional regulation.In all studied cases of completed suicide among women, the results of comprehensive forensic medical examinations were additionally analyzed to ensure the accuracy and objectivity of forensic diagnostic conclusions (Fig. 1).
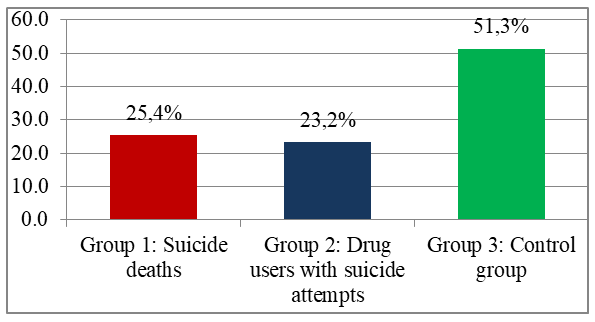 | Figure 1. Distribution of women by study groups according to suicidal risk and outcomes |
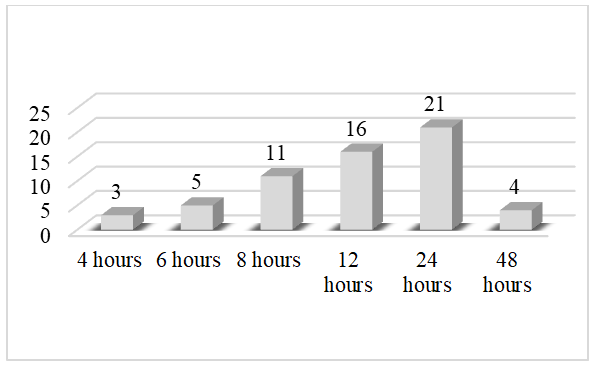 | Figure 2. Cases examined within 48 hours after the incident |
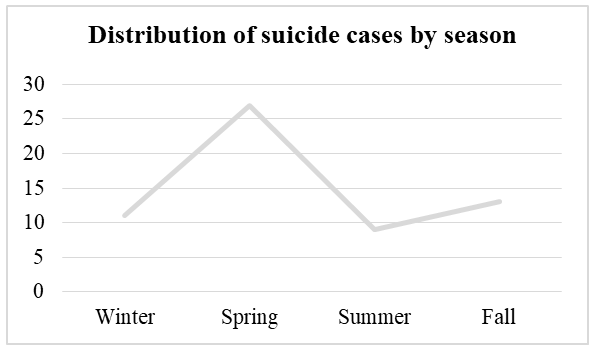 | Figure 3. Analysis of suicide cases by season |
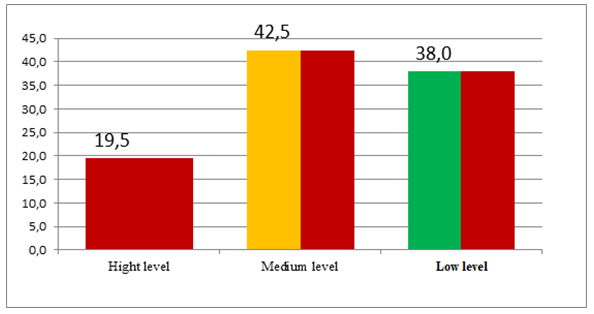 | Figure 4. Level of suicidal tendency |
|
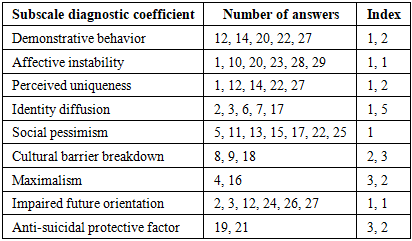
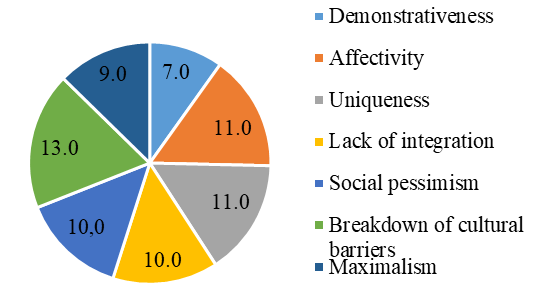 | Figure 5. Distribution of psychosocial factors associated with suicidal risk |
4. Conclusions
- The results of the present study support the feasibility and diagnostic value of implementing systematized forensic medical criteria for the assessment of suicidal behavior in women. A comprehensive evaluation integrating morphological findings, circumstantial evidence, and medico-biological indicators ensures a higher level of objectivity and reliability of forensic conclusions.The proposed multidisciplinary approach may be recommended for routine application in forensic medical practice to improve differentiation of suicide from accidental and non-violent deaths and to enhance the evidentiary quality of expert opinions.