-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(1): 175-179
doi:10.5923/j.ajmms.20261601.39
Received: Dec. 23, 2025; Accepted: Jan. 12, 2026; Published: Jan. 20, 2026

Modern Forensic Approaches to the Diagnosis of Sudden Cardiac Death
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLBobir Sobirovich Turonov1, Gulbahor Bakhshillaevna Juraeva2
1Republican Scientific and Practical Center for Forensic Medicine, Uzbekistan
2Tashkent State Medical University, Tashkent, Uzbekistan
Correspondence to: Gulbahor Bakhshillaevna Juraeva, Tashkent State Medical University, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This article analyzes the role of modern imaging techniques and the significance of morphological findings in the forensic investigation of sudden cardiac death (SCD). SCD is characterized by a high frequency of fatal outcomes occurring within a short period following the onset of initial symptoms, or in their absence. A significant challenge in forensic practice arises when macroscopic autopsy findings are inconclusive. Contemporary approaches to the postmortem diagnosis of SCD integrate morphological, histological, and immunohistochemical analyses. The identification of signs of acute myocardial ischemia, cardiomyopathy, channelopathies, and substrates for ventricular fibrillation is of particular importance. The development and implementation of standardized postmortem diagnostic algorithms can improve the accuracy of cause-of-death determination, especially in young individuals.
Keywords: Sudden cardiac death, Forensic examination, Myocardial infarction, Cardiomyopathy, Morphology
Cite this paper: Bobir Sobirovich Turonov, Gulbahor Bakhshillaevna Juraeva, Modern Forensic Approaches to the Diagnosis of Sudden Cardiac Death, American Journal of Medicine and Medical Sciences, Vol. 16 No. 1, 2026, pp. 175-179. doi: 10.5923/j.ajmms.20261601.39.
1. Introduction
- Sudden cardiac death (SCD) remains a leading cause of mortality worldwide, particularly among young adults. Modern research emphasizes the molecular and genetic underpinnings of SCD, offering new perspectives for forensic diagnostics. In economically developed countries, the annual incidence of SCD ranges from 18.6 to 128 cases per 100,000 inhabitants [1,2]. Epidemiological data indicate that ischemic heart disease (IHD) is the predominant cause of SCD overall. In individuals under 45 years of age, SCD is most frequently associated with various forms of cardiomyopathy. In an analysis of deaths in persons under 35, Andersson, Vasan, et al. found that IHD and cardiomyopathy accounted for a significant and comparable percentage of SCD cases [3,4,5]. Postmortem genetic analyses have revealed that in up to 40% of SCD cases attributed to cardiomyopathy, mutations were identified in genes responsible for cardiac structural proteins, while in 60%, mutations were found in genes related to ion channel function and electrolyte metabolism [6,7]. It is also noted that impaired cardiac conduction can result from mutations in genes encoding desmosomal proteins [8,9].According to World Health Organization statistics, cardiovascular diseases (CVDs) accounted for 30% of all global deaths in 2008, amounting to 17.3 million lives lost; of these, 7.3 million deaths were due to IHD and 6.2 million to stroke. Projections suggest that by 2030, approximately 23.6 million people will die from CVDs annually, with heart disease and stroke likely remaining the leading causes [WHO].In forensic practice, the primary criteria for determining the cause of sudden death are the macroscopic and microscopic findings from autopsy, aimed at identifying significant morphological alterations in organs and tissues [10,11,12]. However, a comprehensive understanding of the clinical, morphological, and molecular biological characteristics of various SCD etiologies is required to elucidate its mechanisms fully. Such understanding is crucial for developing effective diagnostic, preventive, and therapeutic strategies. Although modern forensic examination increasingly incorporates advanced laboratory and instrumental techniques, numerous challenges persist, necessitating further research.The purpose: To study the pathomorphological mechanisms of sudden cardiac death and their significance for determining thanatogenesis in forensic medical examination, to improve diagnostic accuracy.
2. Materials and Methods
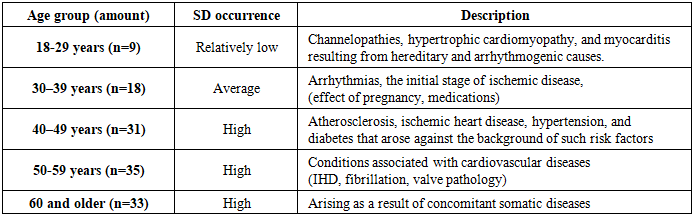
- A clinical, anamnestic, morphological, and statistical study was conducted. The study material comprised 126 autopsy cases from the Republican Scientific and Practical Center for Forensic Medical Examination (Tashkent), collected between 2021 and 2025. The diagnosis of SCD was confirmed based on clinical history and morphological data. During autopsy, tissue samples from all major internal organs, including the heart, were collected for histological examination. Tissue sections were processed using standard methods, embedded in paraffin, and stained with hematoxylin and eosin. All histological slides were examined in detail using light microscopy at 10×, 20×, and 40× magnifications. The most informative and significant pathomorphological changes identified in the heart, lungs, kidneys, and vasculature were documented photographically.
3. Results and Discussion
- Histopathological analysis of myocardial tissue revealed the following characteristic changes (Figure 1): Cardiomyocyte Dystrophy: Pronounced dystrophic changes were observed, including granular and vacuolar degeneration. There was a loss of transverse striation, myolysis, and cytoskeletal disintegration within the cytoplasm. These alterations, which develop in the context of ischemia, hypoxia, and metabolic stress, lead to a complete loss of cardiomyocyte function. Cell Death: Signs of myocytolysis and fragmentation were detected in individual cells, indicating terminal cardiomyocyte injury. Cellular Disproportion: Pathological hypertrophy of some cardiomyocytes contrasted with atrophy in others, suggesting a focal hemodynamic imbalance within the myocardium. Interstitial Edema: Edema of the cardiac interstitium, associated with hypoxic injury and venous congestion, was noted. This leads to stromal loosening, destabilization of tissue architecture, and disruption of intercellular signaling. Microcirculatory Disturbances: Impairments manifested as passive dilation of capillaries and venules, alongside erythrocyte stasis, indicating a severe reduction or cessation of blood flow. These findings are characteristic of acute cardiac decompensation leading to death without resuscitative intervention. The spectrum of morphological abnormalities described was most frequently associated with underlying cardiomyopathies and neurogenic cardiac injury in our series.A review of medical histories, autopsy reports, and ancillary data from the studied cases provided insight into the morphogenetic and pathomorphological changes in parenchymal organs and the cerebral and major systemic vasculature. The analysis confirmed that SCD occurs across all age groups, with varying prevalence and etiological profiles according to age.
|
|
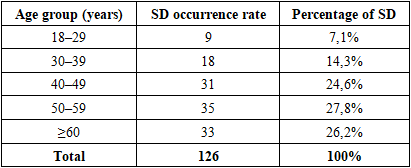
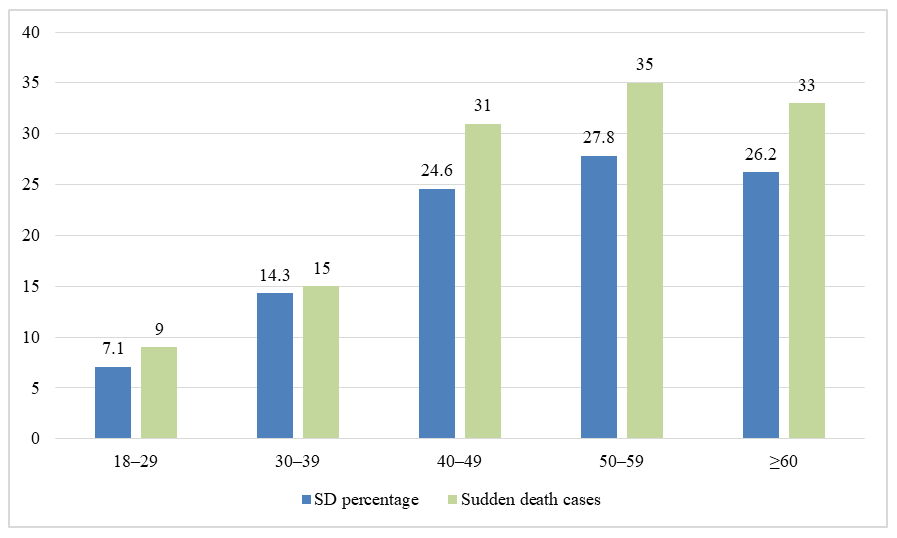 | Diagram 1. Age distribution of sudden death cases and their percentage by age groups |
|
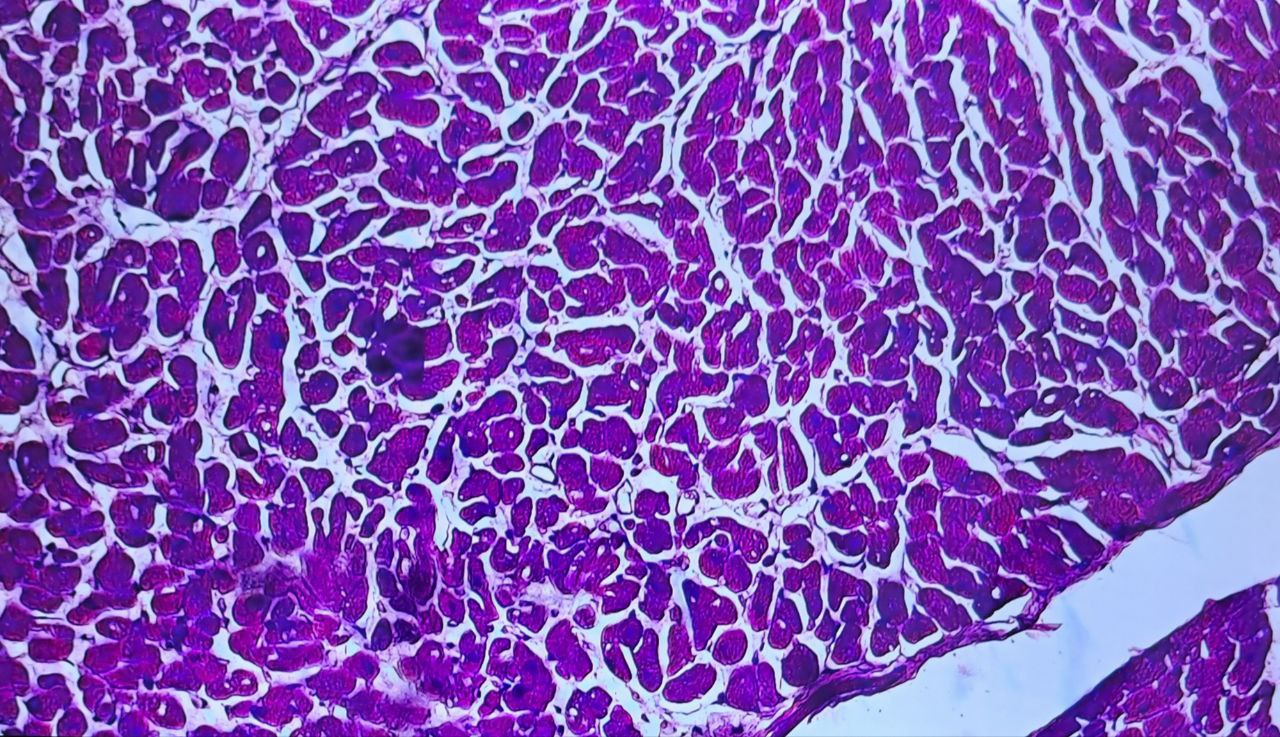 | Figure 1. Cardiomyocytes exhibit marked dystrophic changes, fragmentation, and irregular hypertrophy. The cell cytoplasm shows signs of myolysis, and the stroma displays interstitial edema. The myocardium shows uneven blood filling, paretic dilation of capillaries, and erythrocyte stasis. Stained with hematoxylin and eosin. Magnification 10×20 |
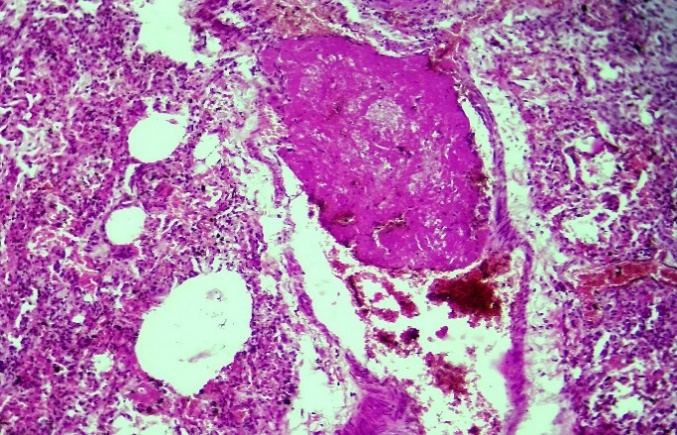 | Figure 2. Sudden death occurred during childbirth due to pulmonary thromboembolism (PTE), with a fibrinous thrombus formed in a major branch of the pulmonary artery; thrombi were also detected in the capillaries. Stained with hematoxylin and eosin. Magnification 10×20 |
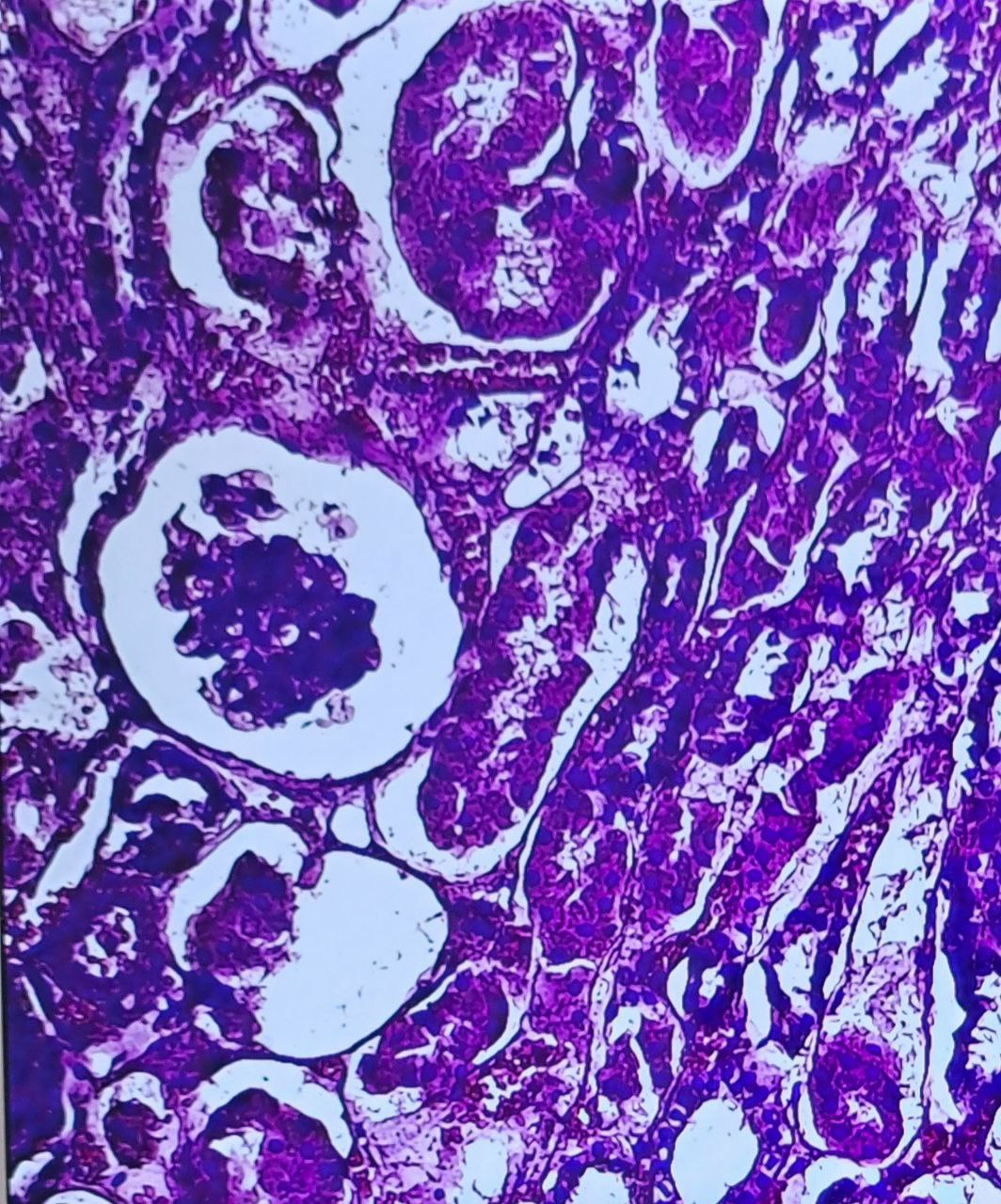 | Figure 3. Sudden death was associated with necrosis of the renal convoluted tubules (a) and atrophy of the glomerular capillary network. (Deceased: male, 34 years old). Stained with hematoxylin and eosin. Magnification 10×20 |
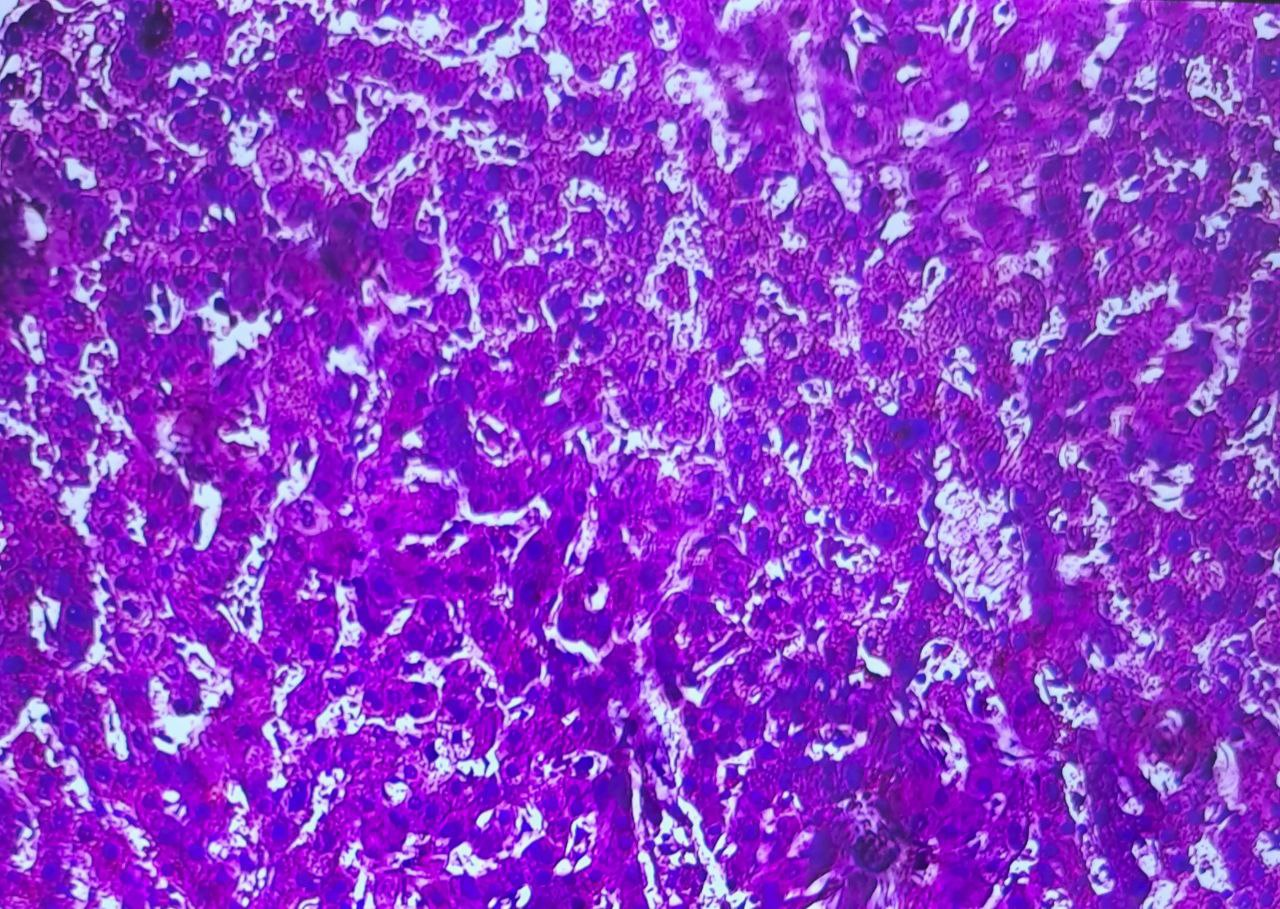 | Figure 4. In a case of sudden death, hepatocytes displayed hydropic and vacuolar degeneration, which developed in the context of acute venous congestion. Stained with hematoxylin and eosin. Magnification 10×20 |
4. Conclusions
- Sudden cardiac death (SCD) remains a leading cause of mortality in the working-age population and poses a significant diagnostic challenge in forensic medicine. Determining the cause of death in such cases necessitates a comprehensive approach, mandating the use of histological and immunohistochemical methods. In this study, the highest incidence of SCD was identified in the 50–59 (27.8%) and ≥60 (26.2%) age groups. The application of modern technologies, such as molecular autopsy and subcellular imaging, significantly enhances pathogenetic analysis and enables the detection of latent hereditary cardiopathologies and channelopathies not apparent on routine macroscopic examination. The standardization of forensic diagnostic algorithms for SCD—incorporating detailed history-taking, clinico-pathological correlation, and integration of advanced laboratory methods—is of paramount importance. In young individuals and in cases without significant atherosclerosis, primary diagnostic focus should be directed toward cardiomyopathies and primary electrical heart disorders. This necessitates close collaboration among forensic experts, geneticists, and pathologists.In summary, the refinement of forensic diagnostic methodologies for SCD, grounded in evidence-based medicine and a multidisciplinary approach, not only clarifies the immediate cause of death but also contributes to preventive strategies for families with a hereditary predisposition.