-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(1): 170-174
doi:10.5923/j.ajmms.20261601.38
Received: Dec. 26, 2025; Accepted: Jan. 17, 2026; Published: Jan. 20, 2026

Pathomorphology of the Adrenal Glands in Preeclampsia
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLEshbaev Erkin Abdukhalimovich1, Roziev Marat Ibodullaevich2
1Doctor of Medical Sciences, DSc., Professor, Department of Pathological Anatomy, Tashkent State Medical University, Tashkent, Uzbekistan
2Independent Researcher, Fergana Institute of Public Health Medicine, Fergana, Uzbekistan
Correspondence to: Eshbaev Erkin Abdukhalimovich, Doctor of Medical Sciences, DSc., Professor, Department of Pathological Anatomy, Tashkent State Medical University, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Preeclampsia is a pathological condition that develops predominantly in the third trimester of pregnancy and whose etiology has not yet been fully elucidated. It is characterized by arterial hypertension, proteinuria, and a range of other clinical manifestations. In preeclampsia, an excessive stress-induced response of the adrenal glands is observed, leading to increased morphofunctional activity and subsequent damage to cellular elements of all adrenal layers. As a result, the adrenal cortex demonstrates pronounced vascular congestion accompanied by focal diapedetic hemorrhages, as well as dystrophic and necrobiotic changes across all cortical zones. Notably, the zona fasciculata of the adrenal cortex is the most vulnerable region; hyperfunctional activity of the glandular epithelium in this zone contributes to the development of massive hyperemia and focal necrosis.
Keywords: Preeclampsia, Adrenal gland, Hyperemia, Necrosis, Necrobiosis
Cite this paper: Eshbaev Erkin Abdukhalimovich, Roziev Marat Ibodullaevich, Pathomorphology of the Adrenal Glands in Preeclampsia, American Journal of Medicine and Medical Sciences, Vol. 16 No. 1, 2026, pp. 170-174. doi: 10.5923/j.ajmms.20261601.38.
Article Outline
1. Introduction
- The relevance of this problem is underscored by the increasing global prevalence of pregnancies complicated by preeclampsia and eclampsia, ranging from 12.3% to 21.3%. In preeclampsia and eclampsia, excessive morphofunctional strain of the adrenal glands leads to disturbances in the sympathoadrenal system [1,2,11]. Consequently, hypertension associated with preeclampsia and eclampsia causes marked vasoconstriction, disrupting the functional relationship between the adrenal glands and the kidneys, which may result in the development of acute renal failure. This emphasizes the clinical and scientific importance of the problem. In the United States and European countries, the prevalence of preeclampsia and eclampsia averages 10.17%, whereas in the CIS countries it reaches 12.1–21.5% [3,4,5]. These conditions are associated with a spectrum of pathomorphological changes in all endocrine organs, including both the cortical and medullary layers of the adrenal glands. Current clinical guidelines for the termination of pregnancy in cases of preeclampsia are largely based on the presence of adrenal insufficiency [6,7,8]. However, to date, comprehensive morphological and morphometric parameters of the adrenal glands in preeclampsia and eclampsia have not been sufficiently established, nor have standardized criteria been developed to support diagnostic and practical recommendations [9,10,12]. This gap highlights the timeliness and significance of the present research topic. From a public health perspective, the preservation and restoration of maternal and child health remains one of the foremost priorities for healthcare systems worldwide, further reinforcing the relevance of this investigation.Objective. To determine the morphological basis of pathological changes occurring in the adrenal glands of pregnant women with preeclampsia and eclampsia during pathological–anatomical diagnosis, with particular emphasis on the mechanisms of thanatogenesis.
2. Materials and Methods
- The study material comprised 32 autopsy cases of women with clinically confirmed diagnoses of preeclampsia and eclampsia who died between 2016 and 2023. All autopsies were performed at the Republican Center of Pathological Anatomy. During the autopsy procedure, adrenal glands were collected from the examined bodies. Morphological examination was carried out using standard hematoxylin and eosin staining. The obtained histological findings were subjected to analytical evaluation and statistical analysis.
3. Results of the Study and Discussion
- Preeclampsia is a multisystem pathological condition that develops in the second half of pregnancy and may persist into the postpartum period. It is characterized by proteinuria, sudden convulsive states, arterial hypertension, and the development of multiple organ failure. Despite extensive research, its etiology remains insufficiently elucidated. As a consequence, premature placental abruption, intranatal fetal death, and disturbances in angiogenic and antiangiogenic factors within the vascular system may occur. In preeclampsia, uneven vascular congestion, dystrophic, and necrobiotic changes develop in all internal organs. In particular, pathological processes involving disruption of integrated regulatory mechanisms between the cortical and subcortical (medullary) regions of the adrenal glands are observed. Frequent fluctuations in blood pressure characteristic of preeclampsia lead to alternating hyperfunction and hypofunction of the cortico–hypothalamic–hypophyseal–sympathoadrenal system. As a result, functional dysregulation occurs, making it difficult to attribute the onset of this pathology to a single etiological factor. Consequently, adrenal dysfunction developing during pregnancy is accompanied by various necrobiotic and hemorrhagic pathomorphological changes. At this stage, it becomes impossible to clearly delineate the specific interrelationships among endocrine glands in pregnancy-associated preeclampsia. From a clinico-morphological perspective, this results in adrenal hyperfunction followed by rapid depletion of the internal reserves of the adrenal cortex. The adrenal capsule generally retains a uniform thickness and is composed of loosely arranged connective tissue. However, uneven vascular congestion and the development of interstitial edema are evident within its vessels. In the studied material, focal petechial hemorrhages in the subcapsular zone of the adrenal gland were identified in an average of 65.7 ± 3.21% of cases, resulting from marked dilation of small capillaries. In areas where petechial hemorrhages were detected, interstitial edema was also observed, extending to adjacent glomerular zones, where pronounced capillary dilation was evident. The presence of uneven, fibrous-layered foci on the capsular surface, along with capsular swelling and destructive defragmentation, was identified in 45.25 ± 3.21% of the examined cases, indicating fibrotic alteration of the capsule. Within the capsule, small foci of developing lymphomacrophage infiltration were noted in perivascular regions, while areas of defragmentation demonstrated proliferative activity of fibroblasts and histiocytes. Additionally, in regions with pronounced interstitial edema, fragmented and loosened collagen fibers were observed, macroscopically confirming adrenal gland swelling. These findings logically support the enlargement of the adrenal glands during the second and third trimesters of pregnancy and their regression to baseline size in the postpartum period. Morphologically, the zona fasciculata of the adrenal cortex demonstrated chromaffin-rich cells containing large inclusions, with prominent fatty dystrophic and necrobiotic changes. Marked capillary congestion, diapedetic hemorrhages, and the development of multifocal necrotic lesions were observed. These alterations contribute to adrenal insufficiency, dysregulation of vascular tone, systemic capillary collapse, and impaired acute perfusion in all vital organs, ultimately leading to the development of multiple organ failure. In the present study, morphological changes characteristic of preeclampsia were found to be largely similar across pregnant women of different age groups, indicating a consistent pattern of adrenal pathomorphological alterations associated with this condition.
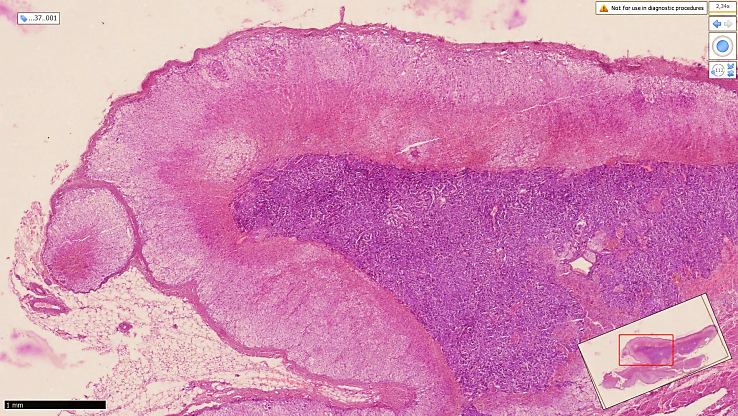 | Figure 3.1. Adrenal gland in preeclampsia from a woman who died at the 35th week of pregnancy. The adrenal gland appears reduced in size against the general background. Marked vascular congestion and interstitial edema are predominantly observed in the zona fasciculata of the adrenal cortex. Necrobiotic changes are identified in the zona glomerulosa. Hematoxylin and eosin staining. Magnification 4 ×10 |
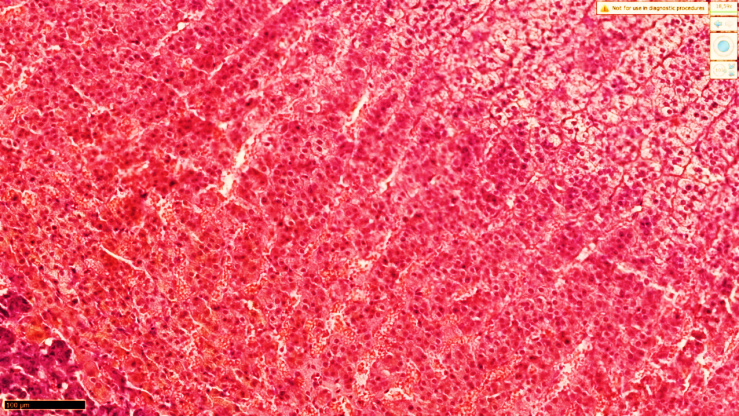 | Figure 3.2. Adrenal gland in preeclampsia. Autopsy of a woman who died at 38 weeks of gestation (Case No. 46 MS). Marked congestion of interstitial capillaries and the development of pronounced interstitial edema are observed in the zona fasciculata of the adrenal cortex (1). The nuclei of the majority of glandular cells are intensely basophilic, which indicates a hyperfunctional state. Hematoxylin and eosin staining. Magnification ×10 ×10 |
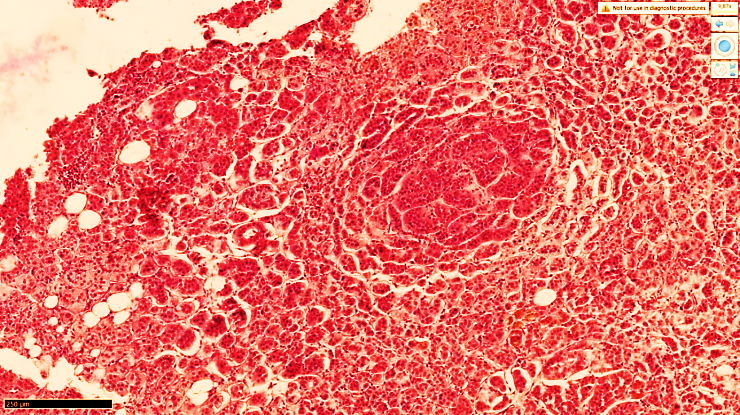 | Figure 3.3. Adrenal gland in preeclampsia. In the zona fasciculata of the adrenal cortex, morphofunctionally activated glandular epithelial cells with a follicular-like arrangement demonstrate extensive necrobiosis and pronounced interstitial edema. Hematoxylin and eosin staining. Magnification 10 ×10 |
 | Figure 3.4. Adrenal gland in preeclampsia from a woman who died at the 36th week of pregnancy. In the zona glomerulosa of the adrenal cortex, dystrophic and necrobiotic changes are identified in epithelial glomeruli of varying sizes. Focal lymphocytic infiltration is observed within the necrotic interstitial stroma. Hematoxylin and eosin staining. Magnification ×20 ×10 |
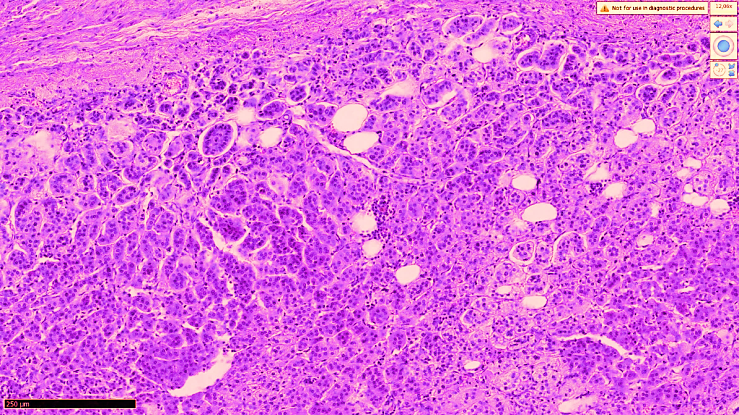 | Figure 3.5. Adrenal gland in preeclampsia from a woman who died at the 34th week of pregnancy. In the zona glomerulosa of the adrenal cortex, microcystic foci of varying size with an emphysematous appearance are observed, along with necrotic glandular epithelial cells and pronounced interstitial edema. Hematoxylin and eosin staining. Magnification ×20 ×10 |
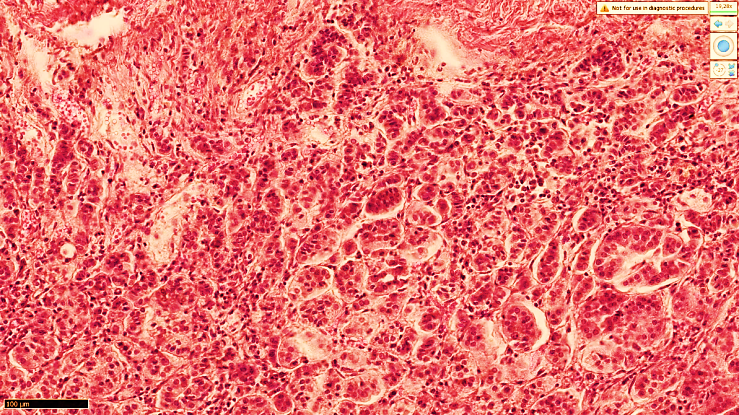
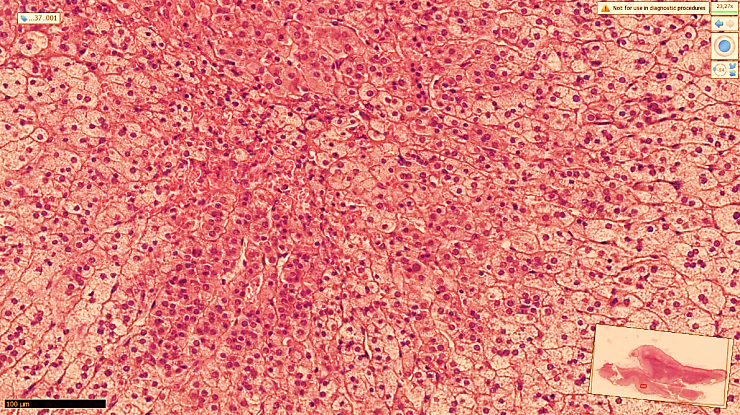 | Figure 3.6. Adrenal gland in preeclampsia. Autopsy report No. 51 MS of a pregnant woman who died at 39 weeks of gestation. In the zona fasciculata of the adrenal cortex, glandular epithelial cells exhibit cytoplasm rich in pale granular inclusions (1). Marked capillary congestion and foci of monocellular necrosis are identified. Hematoxylin and eosin staining. Magnification ×10 ×10 |
4. Conclusions
- Thus, in preeclampsia, one of the most severely affected regions of the adrenal gland is the zona fasciculata of the cortex, where pronounced vascular congestion, dystrophic, and necrobiotic changes develop. These alterations result in functional insufficiency of this zone, accompanied by interstitial edema and foci of diapedetic hemorrhage. Such changes are not exclusively specific to preeclampsia; rather, they reflect sustained arterial hypertension, reduced renal diuresis, and an initial phase of hyperfunctional activity of the zona fasciculata followed by hypofunction and dysfunction. From a pathogenetic standpoint, similar alterations may also be observed in other pathological conditions. However, in the present study, these changes were consistently identified in pregnant women with preeclampsia. In the zona reticularis of the adrenal cortex, morphological changes similar to those described above were also observed, including uneven vascular congestion, extensive interstitial edema between horizontally arranged cuboidal epithelial cells, marked dilation of small capillaries, and the presence of diapedetic hemorrhages. These findings indicate that, in pregnancy-associated preeclampsia, pathological changes predominantly involve the cells located at the boundary between the zona fasciculata and zona reticularis, as well as the upper third of the zona reticularis. In the glandular epithelium of the zona reticularis, an increased number of granular inclusions was also noted. The dense capillary network characteristic of this zone appears to partially compensate for the loss of function of the zona fasciculata. At the same time, extensive dilation of the capillary networks in the zona reticularis leads to congestion of postcapillary venules at the corticomedullary junction, accompanied by interstitial edema and necrotic foci in chromaffin cells of the medulla. These changes are associated with the formation of a mild, locally expressed inflammatory infiltrate. In summary, the main morphological changes identified in the adrenal glands in preeclampsia include the formation of widespread foci of vascular congestion in all cortical zones, capillary paralysis leading to diapedetic hemorrhages, the development of interstitial edema, excessive accumulation of lipid inclusions in glandular epithelial cells of the zona fasciculata, and the progression of dystrophic and necrobiotic changes. The zona fasciculata was the most severely affected cortical region, characterized by multifocal necrotic lesions and the presence of enterchromaffin-like cells of varying sizes rich in lipid inclusions.