-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(1): 166-169
doi:10.5923/j.ajmms.20261601.37
Received: Dec. 26, 2025; Accepted: Jan. 16, 2026; Published: Jan. 20, 2026

Association Between Clinical Factors and Morphological Placental Damage in Premature Placental Abruption in High-Risk Pregnant Women
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLOrtiqova Feruzakhon
Research Fellow, Samarkand Medical University, Samarkand, Uzbekistan
Correspondence to: Ortiqova Feruzakhon, Research Fellow, Samarkand Medical University, Samarkand, Uzbekistan.
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Premature abruption of a normally implanted placenta (placental abruption) was investigated as one of the most severe and prognostically unfavorable obstetric conditions in pregnant women. The aim of the study was to evaluate clinical and morphological factors associated with the development of placental abruption in women at high risk. The material included the results of a comprehensive clinico-morphological analysis of 107 women diagnosed with placental abruption at 28–36 weeks of gestation; the control group consisted of women with a physiological course of pregnancy and delivery. Morphological examination of the placentas revealed characteristic changes, including extensive intervillous hemorrhages, trophoblastic destruction with fibrinoid necrosis, as well as signs of vascular spasm and endothelial dystrophy. The findings indicate that placental abruption is a polyetiological process primarily associated with impaired vascular adaptation and structural alterations of placental tissue, highlighting the future relevance of an integrated clinico-morphological approach for early identification of high-risk patients and prevention of obstetric complications.
Keywords: Premature placental abruption, Risk group, Placental morphology, Placental insufficiency, Ischemia, Vascular disorders
Cite this paper: Ortiqova Feruzakhon, Association Between Clinical Factors and Morphological Placental Damage in Premature Placental Abruption in High-Risk Pregnant Women, American Journal of Medicine and Medical Sciences, Vol. 16 No. 1, 2026, pp. 166-169. doi: 10.5923/j.ajmms.20261601.37.
1. Introduction
- Premature abruption of a normally implanted placenta (PANIP) remains one of the most severe and prognostically unfavorable obstetric complications, accounting for a high level of maternal and perinatal morbidity and mortality [1,2,3]. Despite improvements in antenatal surveillance, intensive care, and obstetric management, the incidence of PANIP shows no consistent tendency toward reduction, while its clinical course is often characterized by sudden onset, rapid progression of complications, and limited possibilities for early diagnosis. A key pathogenetic mechanism of PANIP is an acute disturbance of uteroplacental circulation, leading to the formation of a retroplacental hematoma, pronounced ischemia of placental tissue, and severe fetoplacental insufficiency. However, clinical manifestations frequently do not correlate with the depth and extent of morphological placental damage, which complicates objective assessment of disease severity and prediction of perinatal outcomes [4,5,6]. Complete placental formation, including growth and functional maturation, is achieved by the end of the third month of gestation. During placentation, the functional layer of the endometrium transforms into the decidual membrane, which consists of three parts: decidua basalis, forming the maternal component of the placenta; decidua parietalis, lining the uterine wall free of the embryo and preventing bleeding from lacunae; and decidua capsularis, separating the embryo from the uterine cavity. The basal decidua and capsular layer surround the chorion. In the capsular region facing the uterine cavity, chorionic villi regress and the chorion becomes smooth, whereas in the basal region facing the endometrium, villi undergo intensive branching and development. These villi are immersed in maternal blood-filled lacunae, with some forming anchoring villi that fuse with the basal endometrial layer. Accordingly, the placenta consists of a maternal part (part uterina), represented by the basal decidua and maternal blood lacunae, and a fetal part (part fetalis), represented by the villous chorion. Under modern conditions, morphological examination of the placenta acquires particular importance as an objective method for retrospective verification of PANIP, enabling the identification of both acute and chronic disturbances of placental circulation. Histological analysis allows determination of the temporal characteristics of vascular injury, assessment of ischemic and hemorrhagic changes, and evaluation of the role of vascular, thrombotic, and decidual factors in the development of placental abruption [7,8,9]. Despite numerous publications addressing clinical aspects of PANIP, morphological criteria of this complication remain insufficiently systematized, and their qualitative and quantitative assessment is often fragmentary. Studies based on representative case series with comprehensive morphological characterization of placental tissue are particularly limited, reducing the reproducibility and practical value of available data [10,11,12]. In this context, conducting an in-depth histological investigation of placentas from pregnant women with PANIP based on a substantial clinical dataset represents a highly relevant scientific and practical task. Systematization of morphological features and determination of their diagnostic and prognostic significance will expand current understanding of the pathogenesis of this obstetric complication, improve the accuracy of morphological diagnosis, and provide a foundation for developing objective criteria for assessing the severity of placental insufficiency. The obtained results have future-oriented significance for enhancing clinico-morphological correlations, improving the quality of pathological and forensic medical conclusions, and integrating morphological criteria of PANIP into obstetric and perinatal practice in order to improve maternal and perinatal outcomes.
2. Materials and Methods
- The study was based on the analysis of 107 cases of premature abruption of a normally implanted placenta observed in high-risk women aged 21 to 39 years. The control group consisted of 20 women with a physiological course of pregnancy and delivery. Clinical data included obstetric history as well as the results of laboratory and instrumental examinations (ultrasound, Doppler velocimetry, and coagulation profile). Morphological examination was performed on placental samples obtained after delivery using standard histological techniques with hematoxylin and eosin staining.
3. Results of the Study
- Among the examined women, patients with a complicated course of pregnancy predominated. Arterial hypertension was identified in 20 cases (42.5%), preeclampsia in 17 (36.2%), anemia of pregnancy in 13 (27.6%), and chronic inflammatory diseases of the pelvic organs in 14 women (29.7%). Age over 30 years was noted in 15 patients (31.9%). Signs of placental insufficiency were registered in 18 women (38.3%), manifested by Doppler findings of impaired uteroplacental blood flow, including altered resistance indices of the uterine arteries. In 11 cases (23.4%), premature abruption of a normally implanted placenta was associated with hemostatic disorders and a tendency toward hypercoagulation.Morphological examination revealed characteristic placental changes. Macroscopically, placentas often demonstrated reduced mass and thickness, with areas of hemorrhage and the presence of retroplacental hematomas. In a number of cases, placentas exceeded normal dimensions. On the maternal surface, retroplacental hematomas of varying size, dense or loose consistency, and dark cherry coloration were identified in 43 cases. Tension of the chorionic plate was observed in 15 cases. In 34 cases, placental tissue on section exhibited foci of dark red, brown, or gray-yellow coloration, reflecting ischemic and hemorrhagic alterations.
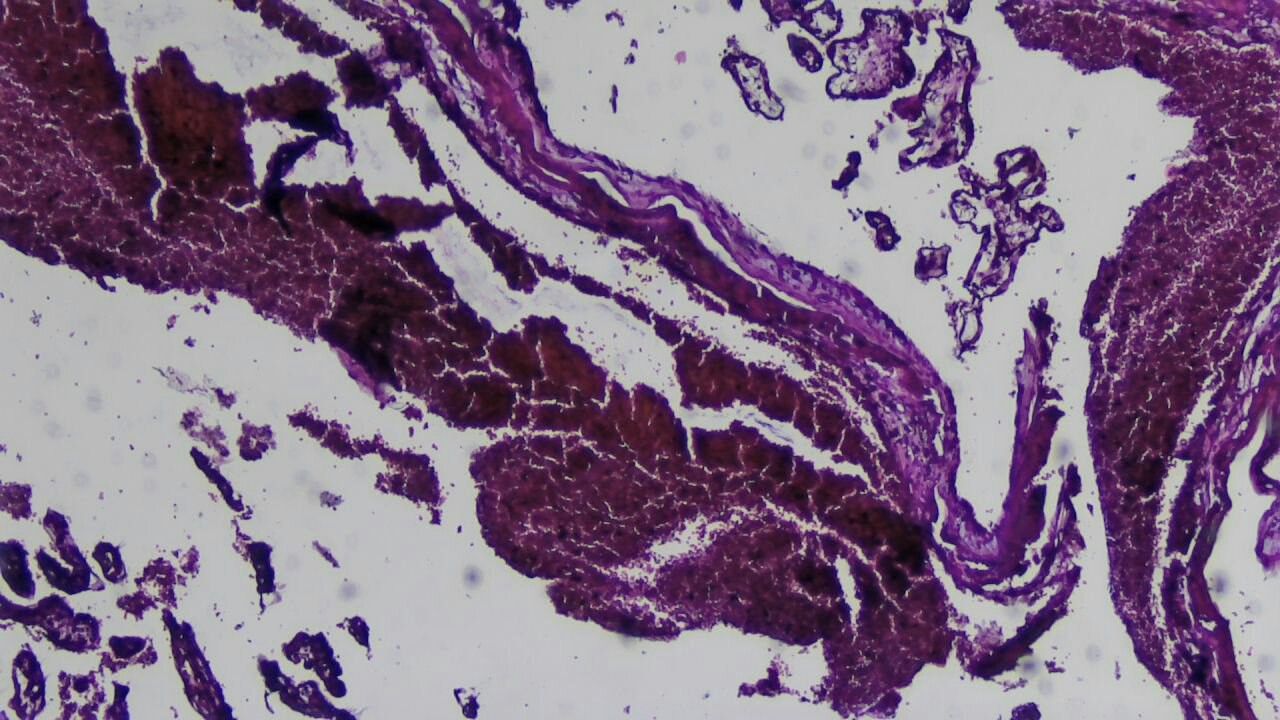 | Figure 1. In the intervillous space, there are extensive accumulations of coagulated and organizing blood, fresh fibrin clots, and areas of organization. Stain: H&E. Magnification: 10x40 |
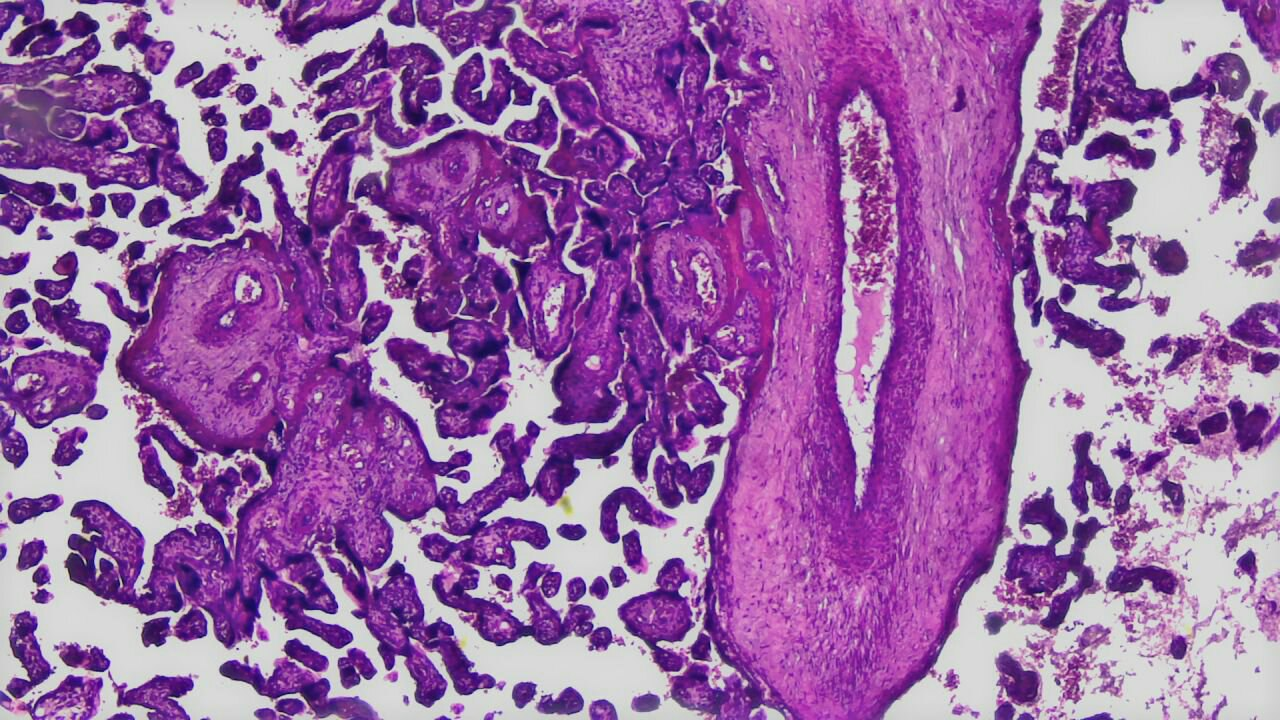 | Figure 2. Formation of a retroplacental hematoma with signs of varying ages, foci of villous compression with deformation of the placental architecture, capillary congestion. Stain: H&E. Mag: 10x40 |
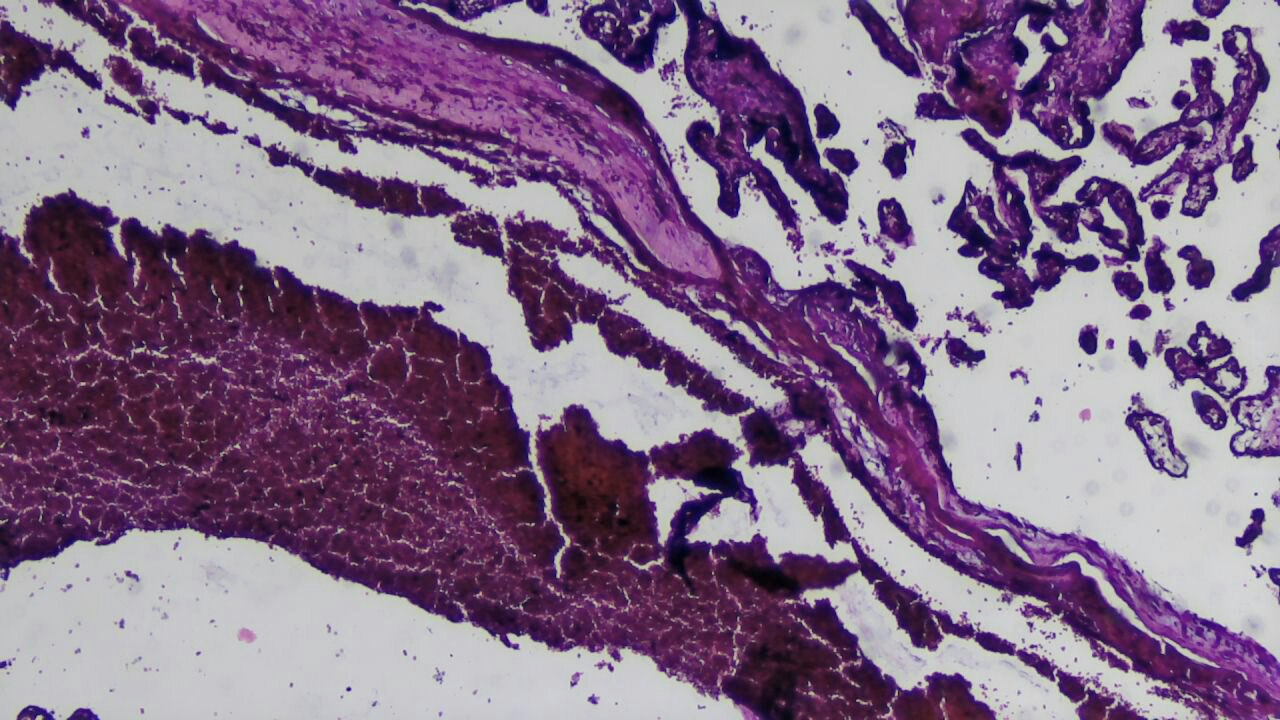 | Figure 3. Extensive hemorrhage in the basal plate, decidual necrosis, damage and ruptures of decidual vessels. Stain: H&E. Mag: 10x20 |
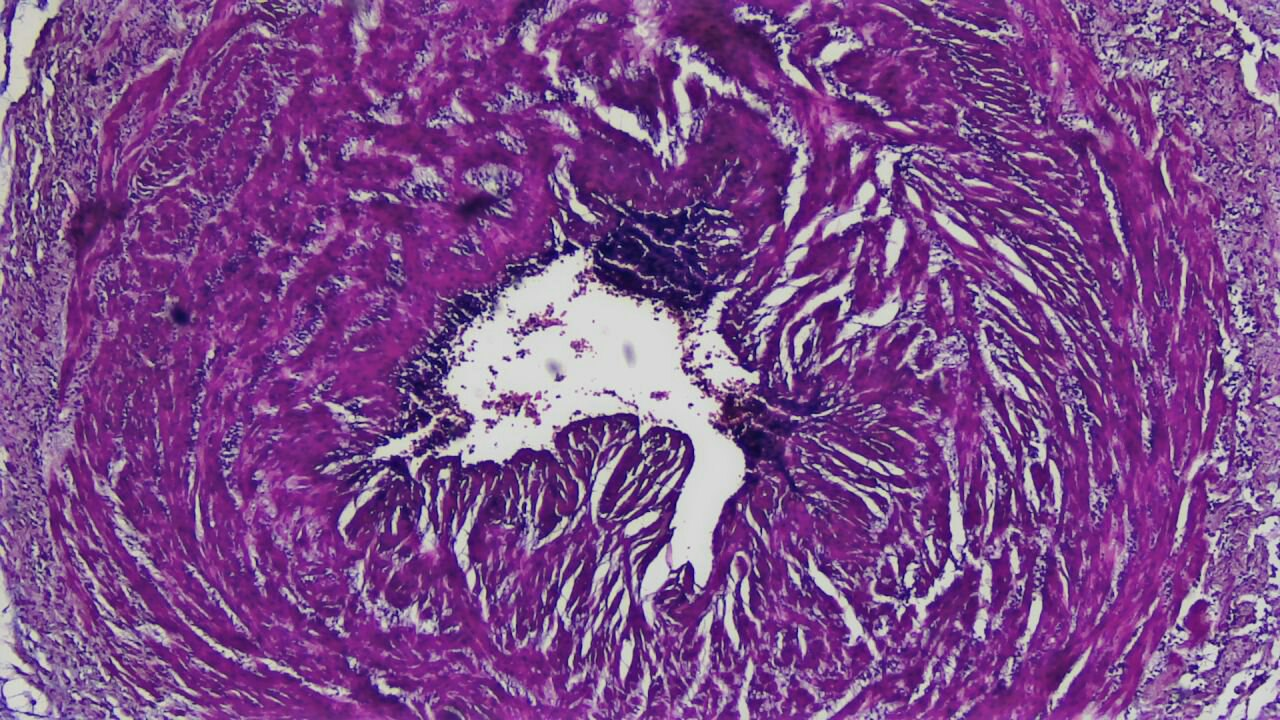 | Figure 4. Extensive intervillous hemorrhages in the placental umbilical cord and pronounced spasm with dystrophic changes of vessels. Stain: H&E. Mag: 10x20 |
4. Conclusions
- Premature detachment of a normally located placenta in women of the risk group is caused by a combination of systemic vascular, inflammatory, and metabolic disorders. The morphological structure of the placenta in PONRP is characterized by ischemic, necrotic, and fibrinoid changes in the chorionic villi, as well as signs of chronic inflammation. Clinical-morphological evaluation of the placenta allows identifying women at high risk and applying differentiated preventive measures to reduce the frequency of obstetric complications.