Usmonalieva B. V.1, Ubaydullaeva Z. I.2
1DSc., Professor, Center for the Development of Professional Qualification of Medical Workers, Tashkent, Uzbekistan
2PhD-Student, Center for the Development of Professional Qualification of Medical Workers, Tashkent, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
This retrospective observational study assessed the prevalence and age-related distribution of serological markers of hepatitis B virus (HBV) and hepatitis C virus (HCV) among blood donors. A total of 45,643 donors examined during 2021–2022 were included in the analysis and stratified according to age groups. The evaluation comprised the detection of HBsAg, antibodies to hepatitis B core antigen (anti-HBc), antibodies to hepatitis B surface antigen (anti-HBs), and anti-HCV, as well as the analysis of combined serological profiles. The results demonstrated a low overall prevalence of HBsAg, consistent with donor population characteristics, while a substantially higher frequency of anti-HBc positivity was observed, increasing progressively with age. Younger donor groups were characterized by a higher prevalence of isolated anti-HBs positivity, reflecting the impact of vaccination programs, whereas older age groups showed a predominance of markers indicating previous exposure to HBV. Combined detection of anti-HBc and anti-HBs was more frequent among donors aged over 35 years, suggesting resolved infection with persistent immunological memory.
Keywords:
Hepatitis B virus, Hepatitis C virus, Blood donors, Serological markers, HBsAg, anti-HBc, anti-HBs, anti-HCV, Age distribution, Epidemiology
Cite this paper: Usmonalieva B. V., Ubaydullaeva Z. I., Frequency and Age-Related Patterns of Hepatitis B and C Serological Markers in Blood Donor Populations, American Journal of Medicine and Medical Sciences, Vol. 16 No. 1, 2026, pp. 157-161. doi: 10.5923/j.ajmms.20261601.35.
1. Introduction
Viral hepatitis B (HBV) and hepatitis C (HCV) remain among the most significant global public health challenges and continue to pose a serious threat to transfusion safety. According to the World Health Organization, approximately 296 million people worldwide live with chronic HBV infection and about 58 million with chronic HCV infection, many of whom remain undiagnosed due to asymptomatic or latent disease courses [1,2]. Blood transfusion is recognized as one of the critical routes of viral transmission in the absence of effective donor screening strategies, making continuous epidemiological monitoring of viral hepatitis markers among blood donors an urgent priority.Despite the widespread implementation of serological screening for hepatitis B surface antigen (HBsAg) and antibodies to HCV (anti-HCV), increasing attention has been directed toward individuals with serological profiles indicative of previous or occult infection. In particular, donors who are HBsAg-negative but anti-HBc-positive may represent a hidden reservoir of HBV infection and a potential residual risk for transfusion-transmitted hepatitis [3,4]. The epidemiological significance of anti-HBc positivity is especially pronounced in regions with intermediate or high HBV endemicity, where exposure to the virus often occurs before the introduction of universal vaccination programs [5].Age-related patterns in the distribution of hepatitis markers provide important insights into the dynamics of infection and the long-term impact of immunization strategies. Numerous studies have demonstrated that younger donor cohorts tend to show higher rates of isolated anti-HBs positivity, reflecting vaccination-induced immunity, whereas older age groups more frequently exhibit serological markers of past natural infection, including anti-HBc with or without anti-HBs [6,7]. These findings underscore the necessity of age-stratified analysis to accurately assess epidemiological trends and evaluate the effectiveness of preventive measures.Hepatitis C virus infection remains another major concern in transfusion medicine. Although anti-HCV screening has substantially reduced the risk of transmission, a considerable proportion of anti-HCV–positive donors may harbor active infection, as evidenced by detectable HCV RNA [8]. Population-based studies indicate that up to 40–60% of anti-HCV–positive individuals remain viremic, highlighting the limitations of antibody-based screening alone and the importance of molecular confirmation [9].In Uzbekistan, data on the age-specific distribution of HBV and HCV serological markers among blood donors are limited, and comprehensive analyses incorporating combined serological profiles remain scarce. Existing screening algorithms are primarily focused on minimal mandatory markers, which may underestimate the true burden of prior exposure to viral hepatitis and obscure important epidemiological patterns. Therefore, a detailed assessment of the prevalence and age-related distribution of HBV and HCV markers among blood donors is highly relevant. Such analysis is essential for optimizing donor screening strategies, improving transfusion safety, and supporting evidence-based public health decision-making aimed at reducing the long-term burden of viral hepatitis.Purpose of the study. was to assess the prevalence and age-related distribution of hepatitis B and C serological markers among blood donors, with particular emphasis on HBsAg, anti-HBc, anti-HBs, and anti-HCV profiles.
2. Materials and Methods
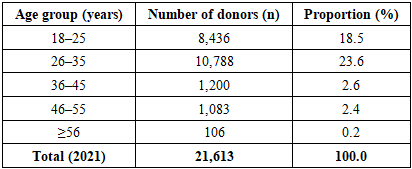
This study was designed as a retrospective observational (cross-sectional) analysis of routine blood donor screening data collected in 2021–2022. The study population included all eligible blood donors who underwent mandatory serological testing for viral hepatitis markers during the specified period. Donors were stratified into predefined age groups (18–25, 26–35, 36–45, 46–55, and ≥56 years) to evaluate age-related distribution patterns (Table 1).Table 1. Characteristics of the study population
 |
| |
|
The study included blood donors who underwent mandatory serological screening for viral hepatitis markers during the study period. Donors were stratified into predefined age groups to assess age-related differences in the distribution of hepatitis B and C markers.Inclusion criteria• Eligibility for blood donation according to national transfusion regulations• Availability of complete serological test results for HBsAg, anti-HBc, anti-HBs, and anti-HCV• Age ≥18 yearsExclusion criteria• Incomplete or missing laboratory data• Repeated donations from the same individual within the same observation periodLaboratory methodsSerological testing was performed using enzyme-linked immunosorbent assay (ELISA) techniques in accordance with manufacturer instructions and national guidelines. The following markers were assessed: hepatitis B surface antigen (HBsAg), antibodies to hepatitis B core antigen (anti-HBc), antibodies to hepatitis B surface antigen (anti-HBs), and antibodies to hepatitis C virus (anti-HCV). Combined serological profiles were analyzed to characterize vaccination-induced immunity, previous exposure, and patterns suggestive of latent infection.Statistical analysisStatistical analysis was performed using standard statistical software. Categorical variables were presented as absolute numbers and percentages. Continuous variables were expressed as mean values with standard error of the mean (M ± m). Comparisons between age groups and between study years were conducted using the chi-square (χ²) test. A p-value of <0.05 was considered statistically significant.
3. Results and Discussion
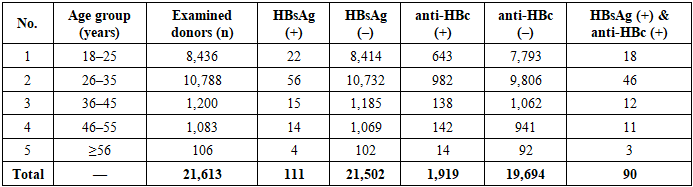
Analysis of serological screening data for 2021 demonstrated a low overall prevalence of hepatitis B surface antigen (HBsAg) among blood donors, consistent with characteristics of a selected donor population. Out of 21,613 examined donors, HBsAg was detected in 111 individuals, corresponding to an overall prevalence of 0.51%. At the same time, antibodies to hepatitis B core antigen (anti-HBc), indicating previous exposure to hepatitis B virus, were identified in 1,919 donors (8.9%), which was substantially higher than the rate of active HBsAg positivity (Table 2).Table 2. Frequency of HBsAg and anti-HBc detection among blood donors in 2021
 |
| |
|
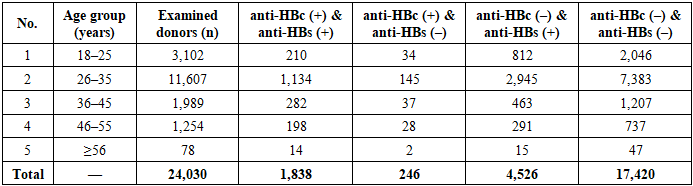
A clear age-related trend was observed for anti-HBc positivity. The prevalence of anti-HBc increased progressively with age, from 7.6% in the 18–25-year age group to 13.2% among donors aged 56 years and older. In contrast, HBsAg positivity showed less pronounced age-related variation, ranging from 0.26% to 3.77%, with slightly higher rates observed in older donor groups.Combined detection of HBsAg and anti-HBc, reflecting active infection with immunological response, was identified in 90 donors, accounting for 81.1% of all HBsAg-positive cases. This finding indicates that the majority of donors with active HBV infection had already developed antibodies to the core antigen, which is consistent with the natural course of HBV infection.Statistical analysis confirmed the significance of age-related differences in anti-HBc prevalence across donor groups (χ² test, p < 0.001). In contrast, differences in HBsAg prevalence between age groups did not reach statistical significance (p > 0.05), reflecting the relatively low number of HBsAg-positive cases in the donor population. These results emphasize that markers of previous HBV exposure accumulate with age, whereas active infection remains relatively infrequent among eligible blood donors. The distribution of combined anti-HBc and anti-HBs serological profiles among blood donors in 2022 demonstrated pronounced age-related differences reflecting both prior exposure to hepatitis B virus and the impact of vaccination programs (Table 3). Table 3. Distribution of blood donors by anti-HBc and anti-HBs serological status in 2022
 |
| |
|
Among 24,030 examined donors, the most frequent profile was the absence of both markers (anti-HBc– / anti-HBs–), which was observed in 17,420 individuals (72.5%), indicating a large proportion of serologically naïve donors.The combination of anti-HBc positivity with anti-HBs positivity, consistent with resolved HBV infection and persistent immunological memory, was identified in 1,838 donors (7.6%). The prevalence of this profile increased with age, from 6.8% in the youngest group (18–25 years) to 17.9% among donors aged 56 years and older, demonstrating accumulation of natural HBV exposure over time.Isolated anti-HBc positivity (anti-HBc+ / anti-HBs–), considered a potentially latent or risk-associated serological pattern, was detected in 246 donors (1.0%). This profile showed a relatively stable but low frequency across all age groups, with a slight predominance among donors aged 26–35 and 36–45 years. Although numerically limited, the presence of isolated anti-HBc is epidemiologically significant, as it may reflect occult HBV infection in a subset of donors.In contrast, isolated anti-HBs positivity (anti-HBc– / anti-HBs+), indicative of vaccination-induced immunity, was observed in 4,526 donors (18.8%). This profile was most prevalent among younger donors, particularly in the 18–25-year age group, where it accounted for 26.2% of cases, and gradually decreased with increasing age, supporting the effectiveness of national immunization programs in younger cohorts.Statistical analysis confirmed a significant association between age group and distribution of serological profiles (χ² test, p < 0.001). Overall, these findings highlight a clear age-dependent shift from vaccine-related immunity in younger donors toward markers of previous natural infection in older age groups, underscoring the heterogeneous immuno-epidemiological structure of the donor population.Analysis of hepatitis C virus markers over the two-year observation period revealed stable detection rates of anti-HCV among blood donors, with minimal year-to-year variation (Table 4). Table 4. Detection frequency of anti-HCV and HCV RNA among blood donors in 2021–2022
 |
| |
|
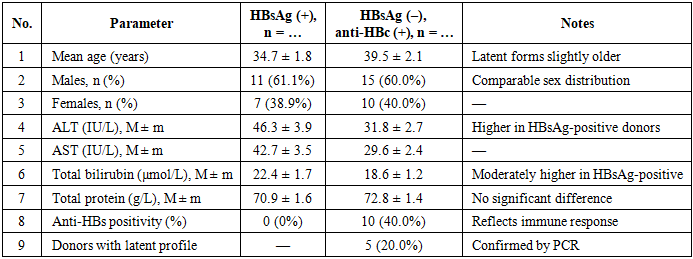
In 2021, anti-HCV antibodies were identified in 142 out of 21,613 donors, corresponding to a prevalence of 0.66%. In 2022, anti-HCV positivity was detected in 156 of 24,030 donors (0.65%). The difference between years was not statistically significant (p > 0.05), indicating a stable epidemiological situation with regard to HCV exposure in the donor population.Among anti-HCV–positive donors, molecular testing demonstrated that a substantial proportion had detectable HCV RNA, indicating active infection. In 2021, HCV RNA was detected in 64 of 142 anti-HCV–positive donors (45.1%), while in 2022 RNA positivity was observed in 71 of 156 donors (45.5%). The proportion of viremic individuals among anti-HCV–positive donors remained consistent between the two years, with no statistically significant differences (p > 0.05).Overall, across the two-year period, anti-HCV antibodies were detected in 298 of 45,643 donors (0.65%). Of these, 135 donors (45.3%) demonstrated detectable HCV RNA, whereas 163 donors (54.7%) were RNA-negative, reflecting either resolved infection or non-viremic status at the time of screening. The stability of both anti-HCV prevalence and RNA positivity rates suggests persistent circulation of HCV at a relatively constant level within the donor population.These findings underscore the epidemiological importance of confirmatory molecular testing in anti-HCV–positive donors, as nearly half of seropositive individuals were found to have active infection. Reliance on antibody-based screening alone would therefore be insufficient for accurate risk assessment and optimal transfusion safety.Comparative analysis of donors with active hepatitis B infection (HBsAg-positive) and donors negative for HBsAg but positive for anti-HBc revealed distinct clinical and laboratory differences (Table 5). Table 5. Comparative characteristics of HBsAg-positive donors and HBsAg-negative, anti-HBc-positive donors
 |
| |
|
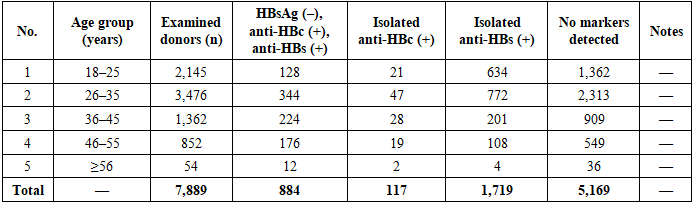
Donors with an anti-HBc–positive, HBsAg-negative profile were slightly older than HBsAg-positive individuals, indicating accumulation of latent or past infection with increasing age. The sex distribution in both groups was comparable, with a predominance of males and no statistically significant differences observed (p > 0.05).HBsAg-positive donors demonstrated significantly higher levels of alanine aminotransferase (ALT) and aspartate aminotransferase (AST) compared with HBsAg-negative/anti-HBc-positive donors (p < 0.05), reflecting more pronounced hepatocellular activity in active infection. Total bilirubin levels were also moderately higher in the HBsAg-positive group, whereas total protein concentrations did not differ significantly between groups.Anti-HBs antibodies were detected exclusively in the HBsAg-negative/anti-HBc-positive group, where they were present in 40.0% of donors, indicating the formation of an immune response after resolved infection. In addition, polymerase chain reaction testing identified latent HBV infection in 20.0% of donors within this group, confirming the presence of occult forms despite the absence of HBsAg.Analysis of combined anti-HBc and anti-HBs profiles among HBsAg-negative donors revealed pronounced age-dependent differences in immunological status and prior exposure to hepatitis B virus (Table 6). Table 6. Frequency of combined anti-HBc and anti-HBs detection among HBsAg-negative blood donors
 |
| |
|
Among 7,889 examined donors, the most prevalent profile was the absence of both markers, observed in 5,169 individuals (65.5%), indicating a large proportion of serologically naïve donors.The combined presence of anti-HBc and anti-HBs, consistent with resolved HBV infection and persistent immune memory, was detected in 884 donors (11.2%). The frequency of this profile increased steadily with age, from 6.0% in the 18–25-year age group to 22.2% among donors aged 56 years and older, reflecting cumulative exposure to HBV over time.Isolated anti-HBc positivity, representing a potentially latent or risk-associated serological pattern, was identified in 117 donors (1.5%). Although this profile was relatively uncommon across all age groups, its presence is epidemiologically relevant due to the potential risk of occult HBV infection.In contrast, isolated anti-HBs positivity, indicative of vaccination-induced immunity, was observed in 1,719 donors (21.8%). This pattern was most frequent in younger donors and demonstrated a gradual decline with increasing age, supporting the protective effect of immunization programs in younger cohorts.Statistical analysis confirmed a significant association between age group and serological profile distribution (χ² test, p < 0.001). Overall, these findings highlight a clear transition from vaccine-related immunity in younger donors to markers of resolved natural infection in older age groups, emphasizing the heterogeneous immunological structure of the donor population.
4. Conclusions
The prevalence of hepatitis B and C markers among blood donors was characterized by a low rate of active infection and a substantially higher frequency of markers indicating previous exposure to hepatitis B virus, particularly anti-HBc, which demonstrated a clear age-related increase.Younger donor cohorts were predominantly characterized by vaccination-associated immunity, reflected by a higher prevalence of isolated anti-HBs positivity, whereas older age groups showed a shift toward combined anti-HBc and anti-HBs profiles, consistent with resolved natural infection.The identified heterogeneity of serological profiles among blood donors highlights the epidemiological significance of age-stratified analysis and supports the need for comprehensive assessment of HBV and HCV markers to optimize donor screening strategies and ensure transfusion safety.
References
| [1] | World Health Organization. (2023). Global hepatitis report 2023. Geneva: WHO. |
| [2] | World Health Organization. (2022). Hepatitis B fact sheet. Geneva: WHO. |
| [3] | Raimondo, G., Locarnini, S., Pollicino, T., Levrero, M., Zoulim, F., & Lok, A. S. (2019). Update of the statements on biology and clinical impact of occult hepatitis B virus infection. Journal of Hepatology, 71(2), 397–408. https://doi.org/10.1016/j.jhep.2019.03.034. |
| [4] | Candotti, D., & Allain, J. P. (2009). Transfusion-transmitted hepatitis B virus infection. Journal of Hepatology, 51(4), 798–809. https://doi.org/10.1016/j.jhep.2009.05.020. |
| [5] | Fopa, D., Candotti, D., Tagny, C. T., Doux, C., Mbanya, D., & Allain, J. P. (2019). Occult hepatitis B infection among blood donors from a highly endemic area. BMC Infectious Diseases, 19, 313. https://doi.org/10.1186/s12879-019-3926-9. |
| [6] | Seo, S. I., Kim, H. S., Kim, J. H., et al. (2018). Prevalence and clinical significance of anti-HBc positivity in blood donors. Journal of Viral Hepatitis, 25(3), 292–300. https://doi.org/10.1111/jvh.12821. |
| [7] | Minuk, G. Y., Sun, D. F., Uhanova, J., et al. (2020). Occult hepatitis B virus infection in a North American blood donor population. Canadian Journal of Gastroenterology and Hepatology, 2020, 1–7. https://doi.org/10.1155/2020/8890134. |
| [8] | Stramer, S. L., Dodd, R. Y., & Katz, L. M. (2011). Emerging infectious disease screening in blood donors. Transfusion, 51(7), 1359–1370. https://doi.org/10.1111/j.1537-2995.2011.03120.x. |
| [9] | Laperche, S., Tiberghien, P., Roche-Longin, C., et al. (2017). Fifteen years of HCV nucleic acid testing in blood donors. Transfusion Clinique et Biologique, 24(3), 201–207. https://doi.org/10.1016/j.tracli.2017.05.004. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML