-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(1): 153-156
doi:10.5923/j.ajmms.20261601.34
Received: Dec. 12, 2025; Accepted: Jan. 8, 2026; Published: Jan. 20, 2026

Prevalence and Clinical–Socio-Demographic Characteristics of Emerging Polycystic Ovary Syndrome in Adolescent and Young Female Populations
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKurbanova Z. Sh.1, Ikhtiyarova G. A.2
1DSc., Professor, Bukhara State Medical Institute, Bukhara, Uzbekistan
2PhD Student, Bukhara State Medical Institute, Bukhara, Uzbekistan
Correspondence to: Ikhtiyarova G. A., PhD Student, Bukhara State Medical Institute, Bukhara, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This clinical observational study assessed the clinical, socio-demographic, and lifestyle characteristics of adolescents and young women with emerging polycystic ovary syndrome (ePCOS). A total of 150 participants aged 16–25 years were examined and stratified into two clinical groups with ePCOS and a control group of healthy individuals. The assessment included age distribution, anthropometric parameters, menstrual cycle characteristics, lifestyle-related risk factors, and socio-clinical indicators. The results demonstrated a high prevalence of menstrual irregularities, including oligomenorrhea and cycle instability, among girls with ePCOS compared to controls. Participants in the primary group were characterized by increased body mass index, a high frequency of abdominal obesity, and a predominance of sedentary lifestyle, irregular sleep patterns, frequent fast-food consumption, and chronic stress exposure. In addition, a significant association was observed between hereditary predisposition to obesity and the severity of clinical manifestations of ePCOS. Phenotypic analysis revealed a predominance of hyperandrogenic and metabolic phenotypes among affected individuals. These findings indicate that emerging polycystic ovary syndrome in adolescents and young women is closely associated with adverse socio-clinical and lifestyle factors, emphasizing the importance of early identification and preventive interventions aimed at modifying risk factors at a young age.
Keywords: Emerging polycystic ovary syndrome, Adolescents, Young women, Socio-demographic characteristics, Lifestyle factors, Menstrual disorders, Obesity, Phenotypes
Cite this paper: Kurbanova Z. Sh., Ikhtiyarova G. A., Prevalence and Clinical–Socio-Demographic Characteristics of Emerging Polycystic Ovary Syndrome in Adolescent and Young Female Populations, American Journal of Medicine and Medical Sciences, Vol. 16 No. 1, 2026, pp. 153-156. doi: 10.5923/j.ajmms.20261601.34.
1. Introduction
- Polycystic ovary syndrome (PCOS) is one of the most common endocrine disorders affecting women of reproductive age, with a global prevalence ranging from 6% to 15% depending on diagnostic criteria [1]. In recent years, increasing attention has been directed toward the early and “emerging” forms of PCOS in adolescents and young women, as clinical and metabolic disturbances often begin several years before the establishment of classical diagnostic features [2]. According to epidemiological data, menstrual irregularities, hyperandrogenic manifestations, and metabolic risk factors are frequently detected during adolescence, suggesting that PCOS is a progressive condition with early-life origins [3].Large population-based studies indicate that lifestyle-related factors, including sedentary behavior, irregular sleep patterns, unhealthy dietary habits, and chronic psychosocial stress, significantly contribute to the development and progression of PCOS, particularly in young populations [4,5]. Obesity, especially abdominal obesity, is reported in up to 60–70% of patients with PCOS and is closely associated with the severity of clinical manifestations and metabolic disturbances [6]. Moreover, hereditary predisposition to obesity and metabolic disorders further increases the risk of early onset and unfavorable course of PCOS [7].Despite growing evidence of the clinical and socio-demographic determinants of PCOS, data focusing specifically on adolescents and young women remain limited, particularly in terms of structured assessment of lifestyle factors and phenotypic variability [8]. Early identification of socio-clinical risk profiles is essential, as untreated emerging PCOS is associated with long-term reproductive, metabolic, and cardiovascular complications, including infertility, type 2 diabetes mellitus, and dyslipidemia [9,10]. Therefore, comprehensive evaluation of clinical, socio-demographic, and lifestyle characteristics in young females with emerging PCOS is highly relevant and represents an important step toward the development of effective preventive and early intervention strategies.Purpose of the study. was to investigate the clinical, socio-demographic, and lifestyle characteristics of adolescents and young women with emerging polycystic ovary syndrome.
2. Materials and Methods
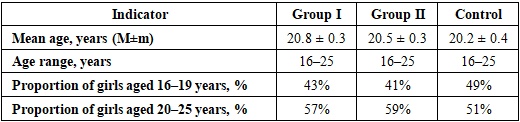
- A clinical observational study was conducted involving 150 adolescents and young women aged 16–25 years. All participants underwent a comprehensive clinical and socio-demographic assessment and were enrolled in the study according to predefined inclusion and exclusion criteria to ensure the homogeneity of groups and minimize the influence of confounding conditions.The study population was stratified into three groups:Group I – girls with emerging polycystic ovary syndrome characterized by pronounced metabolic and clinical manifestations;Group II – girls with emerging polycystic ovary syndrome without marked metabolic disturbances;Control group – apparently healthy girls without clinical or laboratory signs of polycystic ovary syndrome.Age characteristics and population distribution of the examined participants are presented in Table 1.
|
3. Results and Discussion
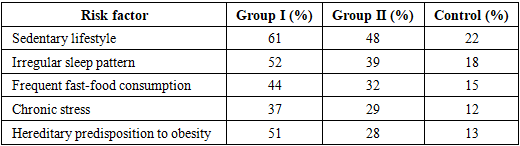
- Analysis of medico-social risk factors revealed a significantly higher prevalence of adverse lifestyle and hereditary factors among girls with emerging polycystic ovary syndrome compared to the control group (Table 2).
|
|
|
|
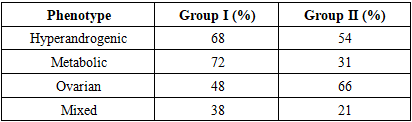
4. Conclusions
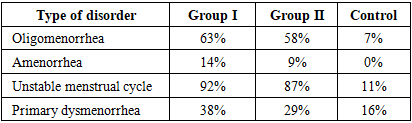
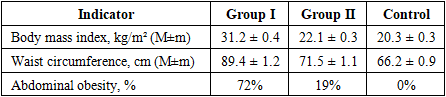
- Emerging polycystic ovary syndrome in adolescents and young women is characterized by a high prevalence of adverse socio-clinical and lifestyle-related factors, including sedentary behavior, irregular sleep patterns, unhealthy dietary habits, chronic stress, and hereditary predisposition to obesity.Girls with emerging polycystic ovary syndrome demonstrate a significantly higher frequency of menstrual cycle disorders and obesity-related anthropometric alterations, particularly abdominal obesity, indicating early metabolic involvement in the disease process.Phenotypic analysis reveals pronounced heterogeneity of emerging polycystic ovary syndrome, with a predominance of hyperandrogenic and metabolically unfavorable phenotypes in girls with more severe clinical manifestations, emphasizing the importance of early identification and individualized preventive strategies.