Rasulov Shokhjakhon Kambarovich1, Khabibova Nazira Nasullaevna2
1PhD Candidate, Bukhara State Medical Institute, Bukhara, Uzbekistan
2DSc, Professor of the Department of Therapeutic Dentistry, Bukhara State Medical Institute, Bukhara, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Local anesthetics are indispensable in modern dental practice, yet adverse reactions, often misinterpreted as allergies, remain a significant clinical challenge. Although true IgE-mediated hypersensitivity to local anesthetics is rare, overdiagnosis is common due to the similarity of allergic reactions to vasovagal, toxic, psychogenic, and adrenaline-related responses. This leads to unnecessary avoidance of effective drugs and increases the risk of complications. Aim. To analyze the clinical features of allergic and pseudoallergic reactions to local anesthetics in dentistry and to identify approaches for optimizing their diagnosis in outpatient settings. Methods. A comprehensive review of current data on the classification of local anesthetics, mechanisms of hypersensitivity, and differential diagnosis of adverse reactions was performed. Special attention was given to the role of structured allergy history, automated questionnaires, and clinical algorithms for risk assessment. Results. True allergic reactions were found to be significantly less frequent than commonly perceived, while most adverse events were associated with non-immunological mechanisms. The use of standardized history-taking tools and automated screening systems improves diagnostic accuracy and reduces false allergy labeling. Conclusion. Accurate differentiation between allergic and non-allergic reactions to local anesthetics is essential for patient safety in dental practice. Implementation of optimized diagnostic algorithms and automated risk-assessment tools allows early identification of high-risk patients and contributes to safer, more effective anesthesia management.
Keywords:
Local anesthetics, Dental anesthesia, Allergic reactions, Hypersensitivity, Differential diagnosis, Vasovagal reaction, Adrenaline effects, Patient safety, Outpatient dentistry, Diagnostic algorithms
Cite this paper: Rasulov Shokhjakhon Kambarovich, Khabibova Nazira Nasullaevna, Clinical Features of Allergic Reactions to Local Anesthetics and Their Frequency in Dental Outpatient Clinics, American Journal of Medicine and Medical Sciences, Vol. 16 No. 1, 2026, pp. 133-137. doi: 10.5923/j.ajmms.20261601.30.
1. Introduction
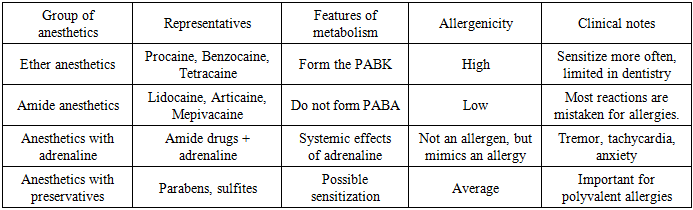
Local anesthetics play a key role in modern dental practice, ensuring the painlessness of most medical and surgical procedures. Despite their widespread use and high safety profile, these medications can cause adverse reactions, including allergic reactions, which often lead to complications during dental appointments. According to the World Allergy Organization (WAO), approximately 40% of the world's population suffers from various allergic diseases, significantly increasing the likelihood of hypersensitivity to medications, including local anesthetics [1,2].Allergic reactions to local anesthetics are considered relatively rare—true allergies occur in only 0.1–1% of patients. However, statistics from dental clinics show that the number of complaints of "allergies" significantly exceeds the actual number of cases. This is because most such episodes are not related to an allergic reaction, but to vasovagal, toxic, psychogenic, or adrenaline effects. Their similarity to the clinical picture of allergies leads to frequent overdiagnosis, unjustified withdrawal of certain medications, and complications in treatment.At the same time, even rare episodes of true allergy can have extremely severe consequences - anaphylactic shock, Quincke's edema, generalized Bronchospasm and other conditions requiring immediate medical attention. Therefore, dentists must be knowledgeable about the risk factors, typical manifestations, and diagnostic algorithms for allergic reactions to ensure maximum patient safety [3].This problem is particularly significant in outpatient dental settings, where the patient is typically not hospitalized and does not have ongoing post-procedure monitoring. In such settings, a proper allergy history, the appropriate choice of anesthetic, timely differential diagnosis, and preparedness for emergency care are crucial.In recent years, interest has grown in the development of automated systems and questionnaires for the preliminary detection of allergic conditions. Such tools allow dentists to quickly and objectively assess the risk of developing hypersensitivity, reduce appointment times, and ensure greater diagnostic accuracy. As demonstrated in a research study conducted at the Bukhara State Medical Institute, the implementation of an automated algorithm for collecting allergy history data contributes to improved safety of dental procedures and a reduced incidence of complications [4,5].Thus, studying the clinical characteristics of allergic reactions to local anesthetics, their actual frequency, and risk factors is a pressing issue in modern dentistry. This article aims to systematize current data on this issue and analyze the possibilities for optimizing diagnostics in dental outpatient settings.Classification of local anesthetics and clinical features of allergic reactionsLocal anesthetics play a key role in dental practice, providing effective pain relief during medical and surgical procedures. However, despite their widespread use and high safety profile, adverse reactions sometimes occur in dental clinics, which patients mistakenly interpret as allergic reactions. To properly assess the risk and guide clinical management, physicians must understand the classification of anesthetics, the mechanisms of hypersensitivity, and the true clinical presentation of allergic reactions.According to modern pharmacological classification, local anesthetics are divided into two main groups— ester and amide —which differ in chemical structure, metabolism, and allergenicity. Ester anesthetics (procaine, benzocaine, tetracaine) are metabolized to form para-aminobenzoic acid (PABA), which has a high sensitizing potential, which explains their relatively high allergenicity. In contrast, amide anesthetics (lidocaine, articaine, mepivacaine, bupivacaine) have a favorable safety profile and rarely cause true allergic reactions, which is why they are used as the drugs of choice in modern dentistry.To clearly present the characteristics of various groups of anesthetics, their metabolism and allergenicity, the classification is given in the table:Table 1. Classification of local anesthetics and their allergenicity
 |
| |
|
Although ether anesthetics have historically been more likely to cause allergic reactions, in modern practice, the vast majority of dental complications are not related to true allergies, but to other conditions that superficially resemble hypersensitivity. However, to properly differentiate, it is necessary to understand the manifestations of a true allergy.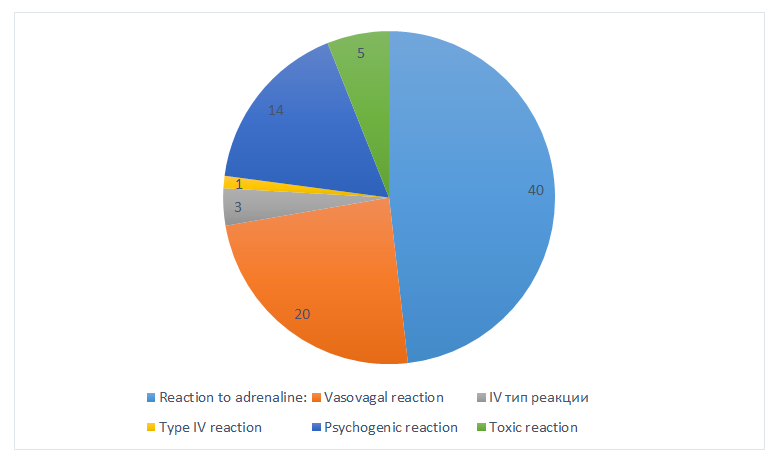 | Figure 1. Actual distribution of reactions mistaken for "allergy to anesthetic" (%) |
True IgE -mediated allergy to local anesthetics is extremely rare but is the most dangerous form. It develops within minutes of drug administration and is characterized by generalized urticaria, itching, angioedema, bronchospasm, severe hypotension, and even anaphylactic shock. These conditions require immediate medical attention. Delayed reactions, on the other hand, occur several hours later and are characterized by local erythema, itching, papular rash, or contact dermatitis. These reactions are most often associated not with the anesthetic itself, but with preservatives and excipients.Much more common in practice are conditions that superficially resemble allergies but are not immunological in origin. These include the vasovagal reaction, which occurs as a result of stress, fear, or painful stimulation. It manifests as sudden weakness, dizziness, pallor, cold sweat, and brief loss of consciousness. Patients often mistakenly attribute this reaction to the administration of anesthetic.No less typical are the symptoms associated with the action of adrenaline, which is found in many cartridges. Increased heart rate, tremors, internal tension, a feeling of fear or heat are often perceived by the patient as an allergy, although in reality they represent a physiological response to the hormone.Toxic reactions associated with accidental intravascular administration or overdose of anesthetic require special attention. They manifest as a metallic taste, tinnitus, tremors, and sometimes seizures. Unlike allergies, toxic effects develop rapidly and require a different treatment approach.Finally, anxious patients often experience psychogenic reactions, including hyperventilation, panic attacks, and a subjective feeling of suffocation. Combined with emotional stress, these can mislead the physician and create the illusion of an allergic reaction.Thus, an analysis of clinical manifestations shows that genuine allergic reactions to local anesthetics are significantly less common than patients assume, while most episodes are the result of vasovagal, adrenaline, toxic, or psychogenic mechanisms. A thorough understanding of these processes allows dentists to accurately assess risks, avoid overdiagnosis, and provide patients with the safest possible treatment conditions.Differential diagnosis of reactions following the administration of local anesthetics is one of the most challenging aspects of a dentist's work, as the clinical presentation of many conditions can resemble an allergic reaction. Correctly distinguishing between true allergies and other similar conditions is vital for choosing safe treatment strategies, preventing complications, and avoiding overdiagnosis, which often leads to unnecessary restrictions on the use of effective medications [5,6].A true allergic reaction develops through an immunological mechanism, most often IgE- mediated, and manifests as systemic symptoms such as urticaria, itching, angioedema, bronchospasm, severe hypotension, or anaphylactic shock. These symptoms develop rapidly, usually within minutes of anesthetic administration, and are progressive. However, in real-life dental practice, the vast majority of episodes misdiagnosed as allergies are not immune-mediated, emphasizing the importance of a comprehensive clinical assessment.One of the most common conditions is a vasovagal reaction, which occurs as a result of severe stress, fear, or emotional overload. It manifests as pallor, cold sweat, dizziness, nausea, a drop in blood pressure, and a brief loss of consciousness. Although symptoms appear immediately after the injection, their mechanism is not related to the anesthetic, but to a reflex response of the autonomic nervous system. A distinctive feature of a vasovagal reaction is bradycardia, whereas tachycardia is usually observed with anaphylaxis [4,6].Reactions caused by adrenaline are also often mistakenly diagnosed as allergies. Because many anesthetics contain a vasoconstrictor, patients may experience increased heart rate, tremors, facial flushing, tension, tremors, and a feeling of apprehension. These symptoms develop rapidly but are not accompanied by a skin rash, bronchospasm, or generalized edema, making them distinguishable from a true allergy. Clinical misdiagnosis often occurs when the patient anticipates a negative outcome and interprets the physiological reaction as a threat.Toxic reactions have a completely different mechanism of development and occur when the anesthetic enters the bloodstream or when the maximum dose is exceeded. A metallic taste, ringing in the ears, agitation, tremors, seizures, or impaired consciousness are typical signs of toxic effects. Unlike an allergy, a toxic reaction occurs almost immediately after intravascular administration and depends on the drug concentration, not the patient's immune sensitivity. Importantly, toxic manifestations are not accompanied by skin symptoms and progress rapidly.Psychogenic reactions, such as panic attacks or hyperventilation syndrome, can also mislead the physician. Due to intense fear or tension, the patient experiences shortness of breath, tingling in the fingers, chest tightness, and a sense of impending "disaster," which they often interpret as an allergy. Unlike a true allergy, there are no skin manifestations, blood pressure is usually elevated or normal, and symptoms subside when the patient calms down and normal breathing is restored [9].Differential diagnosis requires a consistent assessment of the clinical picture, the collected medical history, and the temporal relationship of symptoms to drug administration. True allergic reactions are accompanied by skin manifestations and respiratory disturbances, while non-allergic reactions are accompanied by vascular, emotional, or toxic symptoms. Based on research and observational data, the vast majority of situations perceived as allergies are actually vasovagal, adrenaline, toxic, or psychogenic responses. A clear understanding of the differences between them allows the dentist not only to avoid diagnostic errors but also to ensure maximum patient safety during treatment.Optimizing the diagnosis of allergic reactions to local anesthetics is a priority in modern dental practice, as patient safety and the effectiveness of treatment depend on the accuracy and timeliness of diagnostic procedures. In outpatient settings, where time is limited and many patients experience significant emotional stress, the doctor must have a clear algorithm to avoid errors and differentiate true allergies from non-allergic reactions. The primary goal of optimizing diagnostics is to identify patients at high risk of hypersensitivity before the procedure and prevent the development of life-threatening complications.The first and most important step in diagnosis is collecting a detailed allergy history, which should be completed before the administration of anesthetic. A well-structured interview can identify risk factors, indications of previous drug reactions, the presence of bronchial asthma, atopic dermatitis, hay fever, and other allergic diseases. Assessing past drug intolerances, particularly to anesthetics, antibiotics, and NSAIDs, is crucial. However, in practice, patients often misinterpret their sensations, so the history should be clarified through clarifying questions focused on the nature of the reaction, its duration, and the presence of skin manifestations or systemic disorders. A history of only "palpitations" or "panic" suggests psychogenic or adrenal-related symptoms, not an allergy.Automated questionnaires are becoming increasingly common, significantly simplifying and accelerating the identification of hypersensitivity risks. These questionnaires standardize data collection, eliminate subjective errors, and ensure an objective assessment of the patient's condition. Automated systems, as modern research shows, improve diagnostic accuracy, help dentists make informed decisions, and significantly reduce the likelihood of missing significant risk factors. Their implementation is especially important in busy dental clinics.After collecting the patient's medical history, the dentist should conduct a clinical assessment of the patient's overall condition, including anxiety level, emotional stability, and possible physiological reactions. Patients with high anxiety often exhibit psychogenic reactions that can easily be mistaken for allergies. In such cases, additional explanation of the procedure, breathing techniques, and the creation of a calm environment are recommended. Early identification of anxious patients helps reduce the risk of panic and false reactions during anesthesia.The next step is to determine the need for allergy testing. In most cases, routine skin or provocative testing is not necessary, as true allergic reactions are extremely rare. However, in patients with a significant allergy history or previous reactions to anesthetics, skin testing may be warranted. Lidocaine testing is considered the standard, as it has minimal allergenicity. However, provocative testing should only be performed in a specialized allergy center, as it can provoke a severe reaction.Optimizing diagnostics also includes the mandatory exclusion of non-allergic conditions that superficially resemble allergies. Analyzing the temporal relationship of symptoms, their nature, and dynamics allows the physician to quickly determine whether a vasovagal, toxic, adrenaline, or psychogenic reaction is occurring. A vasovagal reaction is often accompanied by bradycardia and syncope, while an allergic reaction is characterized by tachycardia and skin manifestations. An adrenaline reaction is characterized by no rash, but a sharp onset of tremor and tachycardia. Toxic reactions develop immediately after intravascular administration and are characterized by specific neurological symptoms.An equally important element of an optimized approach is the presence of a clear algorithm for the dentist's actions in the event of a suspected allergy. This includes the following steps: immediately discontinue the drug, assess the patient's vital signs, provide oxygen, place the patient in a horizontal position, and monitor the patient's condition. In cases of true anaphylaxis, administration of epinephrine, antihistamines, and glucocorticosteroids is required, as well as calling an ambulance. Having a pre-prepared emergency kit significantly improves patient safety. Experience shows that most life-threatening complications are not related to the anesthetic itself, but to a delay in providing first aid.An important aspect of optimization is also the selection of the appropriate drug. In patients with a high risk of allergic reactions, drugs containing preservatives and sulfites should be avoided. In such cases, amide anesthetics without additives are preferred. If an injection with a vasoconstrictor is necessary, the patient's individual sensitivity to adrenaline should be taken into account.Thus, optimizing the diagnosis of allergic reactions involves a comprehensive set of measures: a thorough medical history, the use of automated questionnaires, an assessment of the patient's psycho-emotional state, the correct interpretation of symptoms, the selection of a safe medication, and preparedness for emergency care. A clear action plan provides the dentist with confidence in clinical decisions, minimizes diagnostic errors, and creates the safest possible conditions for the patient. In outpatient dentistry, such approaches form the basis for high-quality and modern medical care.
2. Conclusions
An analysis of the clinical characteristics of allergic and non-allergic reactions to local anesthetics in dental outpatient settings suggests that the problem of anesthetic hypersensitivity is significantly exaggerated by both patients and practitioners. True IgE -mediated allergy is rare, while most reactions are associated with vasovagal, psychogenic, toxic, or adrenaline mechanisms. This requires dentists to refine their diagnostic approach rather than adjust their drug selection. A thorough allergy history, accurate assessment of clinical symptoms, and the ability to distinguish true allergies from mimics are key to improving the safety of dental care. The implementation of automated questionnaires and standardized diagnostic algorithms is particularly important, as they help minimize subjective errors, promptly identify at-risk patients, and optimize anesthetic selection. Strict adherence to the physician's protocol, preparedness to provide emergency care, and the necessary equipment enable effective prevention of serious complications and the creation of safe conditions for dental procedures. Thus, optimization of allergic reaction diagnostics is based on a combination of modern clinical knowledge, objective assessment tools, and sound organizational tactics, which together ensure high-quality and safe outpatient dental care.
References
| [1] | Berkun, Y., Ben- Zvi, A., Levy, Y. Evaluation of adverse reactions to local anesthetics // Journal of Allergy and Clinical Immunology. – 2003. – Vol. 112. – P. 143–145. |
| [2] | Bhole, MV, Manson, AL, Seneviratne, SL, Misbah, SA IgE -mediated allergy to local anaesthetics : separating fact from perception // British Journal of Anaesthesia. - 2012. – Vol. 108, No. 6. – P. 903–911. |
| [3] | De Jaco, A., Voltolini, S. Local anesthetic hypersensitivity: Evidence-based evaluation and diagnosis // Allergy. – 2018. – Vol. 73, no. 12. – P. 2432–2440. |
| [4] | Garvey, LH, Kroigaard, M., Poulsen, LK IgE -mediated allergy to local anaesthetics – fact or fiction? // Acta Anaesthesiology Scandinavica. – 2017. – Vol. 61, no. 6. – P. 675–680. |
| [5] | Hepner, DL, Castells, MC Anaphylaxis during the perioperative period. Understanding triggers and management // Anesthesiology. – 2019. – Vol. 130, no. 5. – P. 556–568. |
| [6] | Khabibova NN, Olimova DV Oral hygiene in patients with chronic kidney disease receiving and not receiving hemodialysis: a comparative analysis of traditional and innovative approaches // American Journal of Medicine and Medical Sciences. – 2025. – Vol. 15, no. 3. – P. 542–546. |
| [7] | Malamed, SF Handbook of Local Anesthesia. – 6th ed. – St. Louis: Mosby, 2019. - 432 p. |
| [8] | Olimova DV, Xabibova NN Biochemical analysis of saliva and changes in salivary pH in patients with chronic kidney disease undergoing hemodialysis // New Day in Medicine. – 2025. – No. 1 (75). – P. 415–418. |
| [9] | Speca, SJ, Boynes, SG, Cuddy, MA Allergic reactions to local anesthetic formulations // Dental Clinics of North America. – 2010. – Vol. 54, No. 4. – P. 655–664. |
| [10] | Aksenova, O.V. Allergic reactions to local anesthetics in dentistry: clinical features and diagnostic methods // Russian Dentistry. – 2021. – Vol. 14, No. 4. – P. 22–28. |
| [11] | Mozhaeva, N.N., Fedoseev, G.B. Problems of hypersensitivity to local anesthetics in outpatient dentistry // Clinical immunology and allergology. – 2020. – No. 2. – P. 34-40. |
| [12] | Simbirtseva, N.S., Bortnikova, O.M. Allergic conditions in outpatient dental practice // Bulletin of Dentistry. – 2022. – No. 1. – P. 57–62. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML