-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(1): 66-69
doi:10.5923/j.ajmms.20261601.16
Received: Dec. 23, 2025; Accepted: Jan. 3, 2026; Published: Jan. 9, 2026

Medical, Social and Behavioral Risk Factors for the Development of Hepatopancreatoduodenal System Pathology
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLF. R. Mirzakarimova, A. S. Babadjanov, L. V. Kadomseva
Tashkent State Medical University, Tashkent, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The aim of the study is to investigate the prevalence and role of medical, social, and behavioral risk factors in the development and progression of hepatopancreatoduodenal system pathology based on clinical and statistical analysis. A retrospective study was conducted among 105 patients hospitalized in City Clinical Hospital No. 5 (Tashkent, Uzbekistan) between April and October 2025. The analysis included socio-demographic characteristics, disease structure, dietary habits, psycho-emotional stress, harmful behaviors, medication use, and hereditary predisposition. The most prevalent modifiable risk factors were dry eating habits (65.7%), psycho-emotional stress (57.1%), non-adherence to dietary recommendations (55.2%), uncontrolled use of non-steroidal anti-inflammatory drugs (52.4%), smoking (40%), and alcohol consumption (40%). A substantial proportion of patients belonged to socially vulnerable groups, which was associated with an unfavorable disease course. The results demonstrate the leading role of modifiable lifestyle-related risk factors in hepatopancreatoduodenal pathology and highlight the importance of preventive strategies focused on stress management, dietary correction, and rational medication use.
Keywords: Hepatopancreatoduodenal pathology, Risk factors, Lifestyle, Psycho-emotional stress, Harmful habits
Cite this paper: F. R. Mirzakarimova, A. S. Babadjanov, L. V. Kadomseva, Medical, Social and Behavioral Risk Factors for the Development of Hepatopancreatoduodenal System Pathology, American Journal of Medicine and Medical Sciences, Vol. 16 No. 1, 2026, pp. 66-69. doi: 10.5923/j.ajmms.20261601.16.
1. Introduction
- Diseases of the hepatopancreatoduodenal zone (liver, pancreas, biliary tract, and duodenum) are widespread worldwide and represent a significant medical and social problem. They are characterized by high morbidity and mortality rates, making a substantial contribution to the global burden of disease [1-2]. The high prevalence of these conditions is associated with numerous external and behavioral risk factors [3]. Previous studies have demonstrated chronic stress, unhealthy dietary patterns, harmful habits (such as smoking and alcohol consumption), and uncontrolled use of certain medications play a significant role. It has been shown that psychological stress may independently increase the risk of peptic ulcer disease [4], while for pancreatic cancer the influence of modifiable factors such as tobacco smoking, alcohol abuse, and obesity has been proven [5]. These circumstances emphasize the relevance of studying risk factors in order to develop effective preventive measures.The aim of the study was to investigate the role and prevalence of the main medical, social, and behavioral risk factors (dietary habits, stress, harmful habits, uncontrolled medication use, heredity, etc.) in the development and progression of hepatopancreatoduodenal system pathology based on a clinical and statistical analysis of inpatient data.
2. Material and Methods
- The study was based on an analysis of examination and treatment results of 105 patients with hepatopancreatoduodenal system pathology who were hospitalized in City Clinical Hospital No. 5 from April to October 2025. Among the examined patients, there were 49 (46.7%) women and 56 (53.3%) men; the mean age was 51.14 ± 2.3 years.Clinical and statistical data were collected through a retrospective analysis of medical records (inpatient case histories), as well as patient questionnaires aimed at identifying medical, social, and behavioral risk factors. The obtained data were systematized and processed using SPSS software on a personal computer.
3. Results
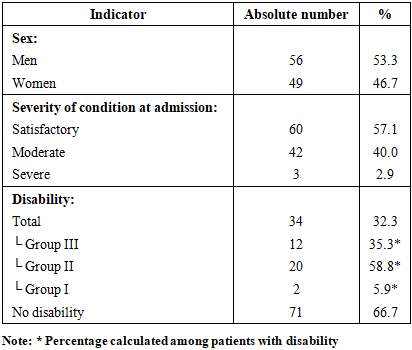
- Analysis of age characteristics showed that the mean age of women was 53.5 ± 2.6 years, while that of men was 46.05 ± 3.2 years. In the overall structure of the examined patients, men predominated – 56 (53.3%), while women accounted for 49 (46.7%). According to the severity of the condition at admission, patients were distributed as follows: 60 (57.1%) patients were admitted in a satisfactory condition, 42 (40.0%) in a moderate condition, and 3 (2.9%) in a severe condition. Disability due to hepatopancreatoduodenal system pathology was observed in 34 (32.3%) patients. Among them, disability group III was established in 12 (35.3%), group II in 20 (58.8%), and group I in 2 (5.9%) patients. In 71 (66.7%) patients, disability was not registered (Table 1).
|
|
|
|
4. Discussion
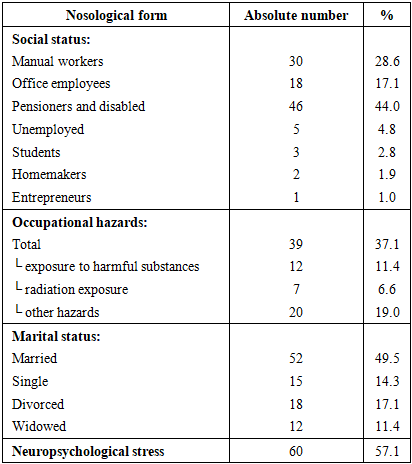
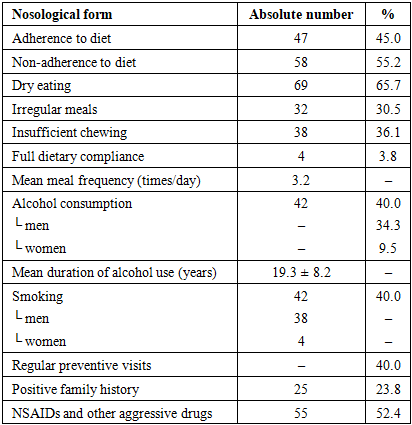
- In the present study, a wide spectrum of medical, social, and behavioral risk factors was identified among patients with hepatopancreatoduodenal pathology. The most prevalent factors were psychoemotional stress (57.1% of exacerbations were preceded by stress), dry eating habits (65.7%), and non-adherence to dietary recommendations (55.2%). In addition, a substantial proportion of patients reported alcohol consumption (40%) and smoking (40%), more than half of the patients (52.4%) used medications aggressive to the gastrointestinal tract (e.g., NSAIDs), 23.8% had a positive family history, and 44% were pensioners or non-working disabled individuals. These findings are largely consistent with data reported in contemporary literature [6], highlighting their relevance and significance.The obtained results confirm the key role of psychosocial stress in the development and exacerbation of gastroduodenal diseases. In more than half of patients, exacerbations were preceded by stress exposure, which is consistent with international studies. Psychological stress may impair gastroduodenal perfusion, reduce mucosal defense mechanisms, and provoke acid hypersecretion, thereby contributing to ulcer formation [7]. Stress is recognized as one of the most common risk factors for peptic ulcer disease. According to a large prospective study, high perceived stress levels are associated with more than a twofold increase in the risk of gastric or duodenal ulcer development [4]. Thus, stress exposure significantly affects the course of hepatopancreatoduodenal pathology, delaying ulcer healing and promoting relapses.Dietary habits also play an important role. The eating pattern disturbances identified in our study—namely dry eating and poor dietary adherence—correlate with findings of international research. Irregular meals, including skipping breakfast and lack of meal regularity, have been shown to significantly increase the risk of dyspepsia and peptic ulcer disease [8]. Regularity and balance of nutrition directly affect the condition of the gastric and duodenal mucosa; insufficient fluid intake and coarse dietary patterns may weaken the gastrointestinal protective barrier. Recent studies report a higher prevalence of gastroduodenal disorders among individuals with irregular eating habits and poor-quality diets [9], which is consistent with the high proportion of patients with dietary нарушения observed in our study.Harmful habits such as alcohol consumption and smoking make a substantial contribution to the pathogenesis of upper gastrointestinal diseases. In our sample, 40% of patients consumed alcohol and the same proportion smoked. These factors are widely recognized as significant risks in international research. Smoking is strongly associated with ulcer formation; global epidemiological analyses indicate that smoking remains a leading risk factor for peptic ulcer disease and related morbidity and mortality. Numerous studies worldwide have confirmed the role of smoking in both ulcer development and its complications. Alcohol abuse is also considered a factor increasing the risk of gastroduodenal damage. Although there is some controversy regarding the effects of moderate alcohol consumption, it is generally accepted that chronic ethanol abuse exerts a damaging effect on the gastric and duodenal mucosa, promoting ulcer formation [10]. Our data on the high prevalence of smoking and alcohol use emphasize the need to address these modifiable factors in prevention and treatment strategies.Medication-related mucosal injury deserves special attention. More than half of the examined patients (52.4%) used drugs aggressive to the gastrointestinal mucosa, primarily nonsteroidal anti-inflammatory drugs. This finding reflects global trends: widespread NSAID use has led to a significant increase in gastroduodenal ulcers and related complications. NSAIDs, along with aspirin, are recognized as leading causes of peptic ulcer disease, especially in elderly patients, and their combination with other risk factors (such as smoking and alcohol) markedly increases the risk [11]. International guidelines emphasize the need for gastroprotective therapy or alternative treatment in high-risk patients receiving NSAIDs, which aligns with our findings.Finally, the unfavorable hereditary and socio-demographic factors identified in our study are also supported by the literature. A positive family history (23.8% of patients) suggests a possible genetic predisposition to gastroduodenal diseases. Several studies identify family history as a significant risk factor for peptic ulcer disease, which may be related to both genetic mechanisms and shared lifestyle factors or transmission of Helicobacter pylori. Older age and low socioeconomic status (a high proportion of pensioners and disabled individuals—44%) are also associated with an increased risk of gastropathy. It is well known that the prevalence of peptic ulcer disease and its complications increases with age. Recent publications report a growing incidence of ulcers and gastrointestinal bleeding among elderly populations, driven by cumulative exposure to risk factors and concomitant therapies such as NSAID use. Social determinants further contribute: low income and unemployment are often associated with unhealthy lifestyles. Populations with low socioeconomic status are more frequently exposed to clusters of harmful factors—smoking, alcohol use, heavy physical labor, poor diet, frequent analgesic use, and stress [7]. This leads to a higher burden of peptic ulcer disease, as reflected in Global Burden of Disease (GBD) data, which show disproportionately high ulcer-related burden in low-income regions [12].
5. Conclusions
- Diseases of the hepatopancreatoduodenal system are predominantly associated with modifiable risk factors, including stress, dietary disturbances, smoking, alcohol consumption, and uncontrolled NSAID use. The high prevalence of these factors among the examined patients indicates the need to strengthen preventive measures and lifestyle modification strategies, particularly among elderly and socially vulnerable populations.