-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(1): 63-65
doi:10.5923/j.ajmms.20261601.15
Received: Dec. 21, 2025; Accepted: Jan. 7, 2026; Published: Jan. 9, 2026

Comparative Evaluation of Various Methods of Myomectomy
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKochieva A. M.
Tashkent State Medical University, Uzbekistan
Correspondence to: Kochieva A. M., Tashkent State Medical University, Uzbekistan.
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

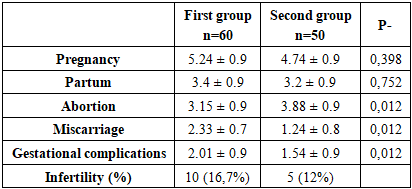
The purpose of the study: To compare various methods of conservative myomectomy surgery and to evaluate the consequences. Materials and methods of the study: We studied the retrospective material of 110 women with uterine fibroids admitted for planned surgical treatment. We divided them into 2 groups: The first group consisted of 60 women who underwent conservative myomectomy surgery using laparoscopic or mini-laparoscopic access, the second group consisted of 50 women who underwent surgery using laparoscopic access. Results: The average number of pregnancies and births exceeded the average estimates, it can be stated that most women had given birth many times. A large number of cases of medical termination of pregnancy can also be noted in both groups. 16.7% of cases in the first group and 12% in the second group had primary or secondary infertility. When analyzing surgical intervention in the women studied, the choice of the surgical method corresponded to the following parameters - anamnesis, complaints, surgical anamnesis, uterine size and size of myomatous nodes. Classification of uterine myoma was carried out according to FIGO 2023. The diagnosis was established on the basis of ultrasound data. Conclusions: When comparing two methods of conservative myomectomy surgery, it is noteworthy that both methods are reliable, depend on the training of the surgeon and the state of the medical equipment.
Keywords: Myoma, Uterus, Laparoscopy
Cite this paper: Kochieva A. M., Comparative Evaluation of Various Methods of Myomectomy, American Journal of Medicine and Medical Sciences, Vol. 16 No. 1, 2026, pp. 63-65. doi: 10.5923/j.ajmms.20261601.15.
1. Relevance
- Uterine fibroids are the most common form of benign, hormone-dependent uterine tumor. According to the WHO, the incidence of uterine fibroids is steadily increasing. The number of surgical interventions is also steadily increasing. Clinical manifestations include abnormal bleeding, the presence of pelvic masses, pelvic pain with specific irradiation, infertility, symptoms of uterine enlargement, and obstetric complications [1,2].Modern treatment strategies primarily involve surgery, but the choice of treatment method is determined by the patient's age and the desire to preserve fertility or avoid "radical" surgery such as hysterectomy. Treatment of uterine fibroids also depends on the number, size, and location of the nodes. Other surgical and nonsurgical approaches include hysteroscopic myomectomy, laparotomy or laparoscopic myomectomy, uterine artery embolization, and radiographic or ultrasound-guided procedures for thermal ablation of uterine fibroids [5,9].Study Objective: To compare various conservative myomectomy techniques and evaluate their outcomes.
2. Study Materials and Methods
- We reviewed a retrospective sample of 110 women with uterine fibroids admitted for elective surgery. We divided the patients into two groups: Group 1, 60 women who underwent conservative myomectomy via laparotomy or minilaparotomy; Group 2, 50 women who underwent laparoscopic surgery. The age range of the subjects ranged from 21 to 44 years. Retrospective material was collected at the Department of Obstetrics and Gynecology of the Tashkent State Medical University, the Jacksoft MDS clinic, and the City Interdistrict Perinatal Center No. 6 of Tashkent.Inclusion criteria for the study groups were:- symptomatic or nodular uterine fibroids- conservative myomectomy surgeries- absence of severe somatic pathologyExclusion criteria were:- gigantic fibroids- hysterectomy surgeries- gynecologic oncologyConservative myomectomy surgery was performed on all women on a planned basis. The surgical approach was selected individually and depended on the woman's preparation, the presence or absence of contraindications, the surgeon's skill, and the woman's wishes.
3. Study Results
- We conducted a thorough comparative analysis of the clinical presentation, medical history, laboratory, and instrumental data of the study women. When analyzing the obstetric and gynecological history, it was noteworthy that all women had a complicated medical history. (Table 1)
|
|
|
4. Conclusions
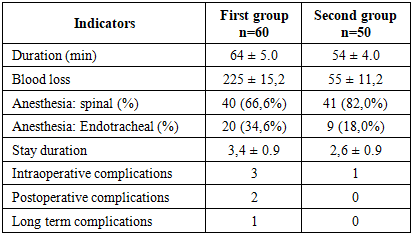
- When comparing the two methods of conservative myomectomy, it is noteworthy that both are reliable and depend on the surgeon's training and the state of the medical equipment. The advantage of the laparoscopic approach is less blood loss and faster patient recovery; the advantage of the laparoscopic approach is its suitability for large adhesions and obesity.