Khakimov M. Sh., Raximzoda T. E., Xabibullayev Sh. A.
Tashkent State Medical University, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Objective: To evaluate the efficacy, safety, and comparative advantages of percutaneous methods in the treatment of liver echinococcosis, considering various cyst types and complications. Materials and Methods: The study included 173 patients with liver echinococcosis treated using percutaneous methods from 2008 to 2021. Patients were categorized into three groups: uncomplicated solitary cysts (135 cases), uncomplicated multiple cysts (12 cases), and complicated cysts (26 cases). The interventions included PAIR (Puncture, Aspiration, Injection, Reaspiration), MoCat (Modified Catheterization), and a staged catheterization technique developed in our clinic. Procedures were performed under ultrasound and fluoroscopic guidance after albendazole chemotherapy. Key outcomes analyzed included cyst involution, residual cavity formation, and complications. Results: Complete involution of residual cavities was achieved in all patients with uncomplicated solitary cysts smaller than 5 cm. Complications were observed in 4.4% of cases in this group, including residual cavities (6 cases) and cyst cavity bleeding (1 case). Among patients with uncomplicated multiple cysts, no significant complications were reported. In the group with complicated cysts, mortality occurred in one case. The staged catheterization technique demonstrated advantages in managing medium to large cysts by effectively addressing issues such as biliary fistulas and incomplete cyst resolution. Conclusions: Percutaneous methods are effective and safe for treating liver echinococcosis, particularly for small and medium-sized cysts. The staged catheterization technique offers significant benefits in managing larger cysts and complications. Combining these methods with conservative and endoscopic interventions provides optimal outcomes for various clinical scenarios.
Keywords:
Liver echinococcosis, Percutaneous treatment, PAIR, MoCat, Staged catheterization, Albendazole chemotherapy, Biliary fistula, Residual cavity
Cite this paper: Khakimov M. Sh., Raximzoda T. E., Xabibullayev Sh. A., Our Experience of Percutaneous Treatment of Liver Echinococcosis, American Journal of Medicine and Medical Sciences, Vol. 16 No. 1, 2026, pp. 45-49. doi: 10.5923/j.ajmms.20261601.12.
1. Introduction
Liver echinococcosis caused by Echinococcus granulosus (cystic echinococcosis) remains one of the most significant problems in medicine, particularly in regions where this parasitic infection is endemic. In some regions, it still remains a public health problem, with approximately 2–3 million cases worldwide and 19,300 deaths annually. In endemic regions, the incidence of human cystic echinococcosis (CE) can exceed 50 cases per year per 100,000 population, with prevalence rates reaching 5–10% in certain parts of Argentina, Peru, East Africa, Central Asia, and China [1]. In Uzbekistan, as in other Central Asian countries, hepatic echinococcosis remains a widespread disease, due to environmental, climatic, agricultural and cultural practices [2].One of the main problems is the diagnosis of this disease, as cysts often remain undetected in their early stages. This leads to patients seeking medical care only when severe symptoms or complications arise. Treatment-related issues are also highly relevant. Surgical cyst removal, traditionally considered the main treatment method, is associated with high risks of complications and mortality [3,4]. In this context, the development and improvement of percutaneous treatment methods gain particular importance. Another critical issue is the prevention of echinococcosis, as the main source of infection is animals, with humans becoming infected through contact or consumption of contaminated food products. Raising public awareness about preventive measures, controlling animal populations, and implementing strategies to prevent infection play a pivotal role in the fight against this disease.Thus, liver echinococcosis remains a pressing problem in Uzbekistan and requires a comprehensive approach that includes not only improved diagnostics and treatment, but also measures to prevent and control the spread of the disease [5,6]. And percutaneous methods of treating liver echinococcosis compared to open surgery are becoming increasingly attractive due to a number of reasons: less invasiveness, shorter hospital stay, less cosmetic defect, low risk of damage to nearby organs, relatively low treatment costs [7].
2. Objective of the Study
The aim of this study is to evaluate the effectiveness and safety of percutaneous methods for treating liver echinococcosis and to select these methods based on the characteristics of different cyst types (single-chamber and multilocular, complicated and uncomplicated), i.e. identifying optimal approaches depending on the features of echinococcal cysts and their possible complications.
3. Materials and Methods
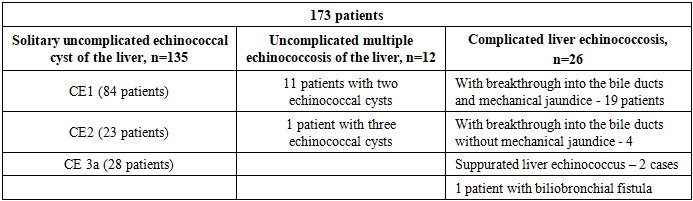
In the Multidisciplinary Clinic of the Tashkent State Medical University, from 2008 to 2021, 173 patients with liver echinococcosis were treated using percutaneous methods. Of these, 135 patients had uncomplicated solitary echinococcal cysts (78%), 12 had uncomplicated multiple hepatic echinococcosis (7%), and 26 had complications (15%) (Table 1). The average patient age was 43 years (range: 18–68 years), with an approximately equal gender distribution (89 men and 84 women, respectively).Table 1. Distribution of patients depending on the type of liver echinococcosis, n=173
 |
| |
|
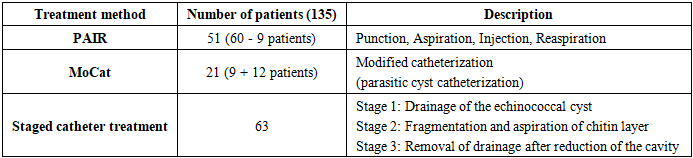
All echinococcal cysts were classified according to the WHO ultrasound classification (2003, 2010) [8,9]. However, following WHO recommendations, patients with class IV and V cysts (calcified, non-viable echinococcal cysts) were not included in the study, as a watch –and-wait approach is recommended for these cases. Informed consent for the procedure was obtained from all patients.Solitary uncomplicated echinococcal cyst of the liverIn both theoretical and clinical practice, early-detected uncomplicated solitary hepatic cysts represent the most suitable group for percutaneous interventions. Since the mid-1990s, numerous variations of percutaneous interventions have been proposed, with most being appropriate for this patients group. The simplest and safest method is PAIR, which remains relevant today. In our clinical practice, in addition to PAIR (51 cases), we also used the MoCat method (21 patients) and a staged catheter treatment method developed within our walls (63 patients).All the above interventions were performed in the X-ray operating room under ultrasound and fluoroscopy guidance. The patients were hospitalized at least one day before the procedure, after a course of albendazole chemotherapy (10–15 mg/kg/day). Preoperative preparation included standard protocols for surgical interventions and standard premedication with the addition of 8 mg of dexamethasone. The presence of an anesthesiologist-resuscitator was mandatory during the operation. The operation was performed under local anesthesia.60 patients with stage I and III A liver echinococcosis underwent the classical percutaneous PAIR method: using a Chibo needle, a cyst puncture was performed under ultrasound control, as much of the cyst contents as possible were aspirated, a hypertonic 20% sodium chloride solution was introduced equal to 2/3 of the aspirated contents, and reaspiration was performed back after an exposure of 7-10 minutes. The operation was performed under fluoroscopy control; upon aspiration of the cyst contents, the fluid in all patients was transparent; no fistulas were detected during fluoroscopy. However, after the onset of the decay of the chitinous cyst membrane, biliary fistulas were detected in 9 cases, after which drainaging of the cyst cavity was performed in this group of patients, i.e. catheterization of the parasitic cyst was performed using the MoCat method.In this case, after the biliary fistula was detected, reaspirated all scolecid saline, a contrast agent was administered for visualization, and the Chibo needle was removed. After that, under the control of fluoroscopy and ultrasound, a puncture was performed with a needle to introduce a 0.035 or 0.038 inch guidewire. After probing the drainage channel, the drainage itself was inserted 9 or 10Fr.Subsequently, in 12 patients, as the primary procedure of choice, catheterization of the parasitic cyst was performed using the MoCat method. In total, drainage of the parasitic cyst using this method was performed in 21 patients with a solitary liver cyst.We have been using the staged drainage method of cystic echinococcosis developed by us since 2014 and it has been performed in 63 patients (Table 2).Table 2. Distribution of patients with solitary uncomplicated liver hydatid disease depending on the treatment method
 |
| |
|
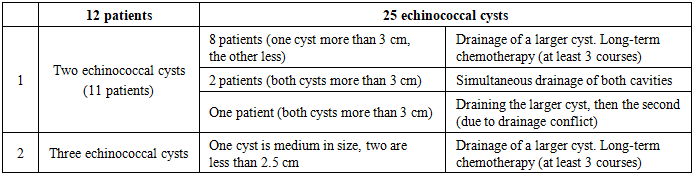
The choice of the above methods was chronological. If at the beginning we used PAIR and MoCat methods, then later we reduced the indications for the PAIR method, and settled on the staged drainage method as the main method of choice. The reason for changing the treatment method was the following:1. PAIR did not completely solve the problem of the residual parasitic cavity, which is expressed in cysts larger than 5 cm (starting from medium cysts). PAIR in the treatment of hydatid disease up to 5 cm, i.e. small cysts, remains a completely effective method.2. Before the destruction of the chitinous membrane with PAIR, we cannot know the presence or absence of a biliary fistula.3. PAIR does not solve the problem of a biliary fistula.4. It is technically difficult to catheterize an echinococcal cyst after disintegration, and the optimal position of the drainage is inside the cavity of the germinal membrane.That is why, due to the ease of implementation and insignificant complications with small cysts, we perform and consider it appropriate to use the PAIR method. For medium and large cysts, preference is given to the staged catheter drainage technique.Uncomplicated multiple echinococcosis of the liverA total of 12 patients with 25 hydatid cysts were treated. In the presence of two cysts larger than 3 cm and smaller than 3 cm, a long course of chemotherapy was performed with drainage of the larger one (8 patients). In two patients with cysts larger than 3 cm, simultaneous drainage of the echinococcal cysts was performed. In one case, due to a conflict in the course of the drainage (the large cyst blocked the small one with its body), staged drainage of the cyst with a larger diameter (8 cm) was performed first, after the reduction of which the smaller one (5 cm) was drained. In a patient with three ECs, only the cyst with a diameter of 5.5 cm was drained (the other two were 1.5 and 2.0 cm) (Table 3).Table 3. Distribution of patients with uncomplicated multiple liver cysts and treatment method
 |
| |
|
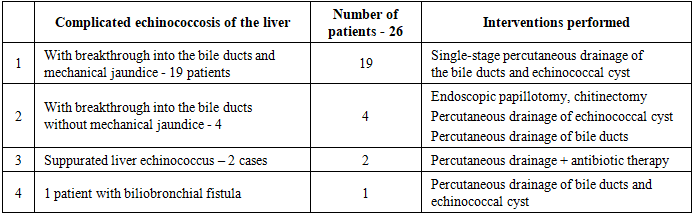
Complicated liver echinococcosisPatients in this subgroup are usually clinically severe patients. In clinical manifestation, depending on the type of complication, they had a number of features. If patients had jaundice after a breakthrough into the bile ducts, and as a rule, most patients sought treatment for the first time and did not indicate echinococcosis in their anamnesis (16 patients - 84%), then they already sought treatment in a severe condition, after visiting authorities (infectious disease specialist, virologist, hepatologist) and with a multiple increase in bilirubin and liver enzymes. Patients with a breakthrough into the bile ducts and without mechanical jaundice were examined for choledochoectasis and the cause was identified during additional examination. Both of the above groups underwent MRI cholangiography to identify the localization and level of obstruction, to determine the treatment tactics. In one case, a patient with a biliobronchial fistula was identified. The anamnesis included two times echinococcectomy from the liver. At the time of his visit to us, the patient had a cough with bile, which reached 100 ml per day (Table 4).Table 4. Distribution of patients with complicated multiple liver cysts depending on the treatment method
 |
| |
|
The management of patients differed according to the subgroups. In case of a rupture into the bile ducts (BD) with mechanical jaundice (MJ), simultaneous drainage of the BD and the echinococcal cyst was performed. In the absence of MJ, chitin layer was removed from the BD endoscopically. Of these, in two cases, after papillotomy, the chitinous membrane was completely removed, after which percutaneous drainage of the cyst was performed with subsequent staged removal of the chitinonus membrane, the drainage tube was removed after the reduction of the residual cavity and complete reduction of bile secretion through the tube. In the remaining two cases, it was not possible to remove the chitinous membrane endoscopically and simultaneous drainage of the EC and BD was performed. Further management of these patients was the same as in the first subgroup, i.e. as with mechanical jaundice.Treatment of patients with a suppurating echinococcal cyst was the same as for a liver abscess. Since the echinococcal cyst is usually dead, these patients did not need chemotherapy, but intensive antibiotic therapy was administered.When identifying a biliobronchial fistula, a thorough approach was important. Of course, one option is performing a radical operation with thoracophrenolaporotomy. However, it is necessary to take into account that a cough with bile indicates a block in the bile ducts, but there is no mechanical jaundice, due to expectoration of bile. And the primary source of all troubles is an echinococcal cyst of the liver, i.e. recurrent EC. Considering all of the above, the patient underwent percutaneous drainage of the bile ducts and echinococcal cyst, after which all of the above symptoms resolved.
4. Results
In patients with uncomplicated solitary cysts up to 5 cm in size, complete involution of the residual cavity occurred. In the late period, after 6 months of observation, one patient developed EC next to the previously existing cyst (apparently along the canal), which was successfully treated with a course of chemotherapy. In 6 patients (3.5%), residual cavity formation was observed: in 4 - clinically not asymptomatic, two patients with suppuration of the residual cavity required repeated drainage with antibiotic therapy. In one patient, bleeding into the cyst cavity was observed during staged drainage (0.6%).In patients with multiple uncomplicated echinococcosis, complications such as anaphylactic reaction, seeding or problematic residual cavity were not observed.In complicated echinococcosis of the liver, one patient died.
5. Discussion
The results of the study show that modern methods of treating echinococcosis are effective and safe for most patients. Complete involution of the residual cavity was achieved in all patients with uncomplicated solitary cysts up to 5 cm. Complications were relatively rare and were successfully treated with additional therapeutic measures. In the group with complicated liver echinococcosis, a higher risk of adverse outcomes was noted, which emphasizes the need for careful monitoring and timely intervention.
6. Conclusions
Percutaneous drainage is an effective method for treating liver echinococcal cysts, especially small and medium cysts. Modern technologies and techniques allow us to constantly improve the results of this procedure, making it increasingly preferable for patients and doctors.Percutaneous methods for treating echinococcosis are becoming increasingly popular due to their minimal invasiveness, high efficiency and short recovery period. Today, there are many variations of percutaneous treatment of echinococcal cysts that can be used at different stages of the life of a parasitic cyst. Naturally, just as there is no cure-all, routine use of a single method promises an unfavorable outcome. Only a combination of the above methods, coupled with conservative, and in some cases combined use of endoscopic and traditional surgical treatment leads to the best results.
References
| [1] | WHO. Echinococcosis: WHO; 2020 (updated in 2024г. https://www.who.int/news-room/fact-sheets/detail/echinococcosis). |
| [2] | Torgerson PR, Oguljahan B, Muminov AE, Karaeva RR, Kuttubaev OT, Aminjanov M, Shaikenov B. Present situation of cystic echinococcosis in Central Asia. Parasitol Int. 2006;55 Suppl:S207-12. doi: 10.1016/j.parint.2005.11.032. Epub 2005 Dec 19. PMID: 16361112. |
| [3] | Vishnevsky V. A., Ikramov R. Z., Kakharov M. A., Efanov M. G. Radical treatment of liver echinococcosis. Current state of the problem // Bulletin of Siberian Medicine 2007, Issue №3. |
| [4] | Kalieva D.K. Echinococcosis. Current issues of surgical treatment // Science and Healthcare 2014, Issue № 6. |
| [5] | Karimov Sh.I., Nishanov Kh.T., Yeshanov A.T., Durmanov B.D. Epidemiological aspects of echinococcosis // Medical Journal of Uzbekistan. - 1997. - No. 3. - P. 59-62. |
| [6] | Babadjanov A.K., Yakubov F.R., Ruzmatov P.Y., Sapaev D.S. Epidemiological aspects of echinococcosis of the liver and other organs in the Republic of Uzbekistan. Parasite Epidemiol Control. 2021 Nov 24; 15: e00230. doi: 10.1016/j.parepi.2021.e00230. PMID: 35005264; PMCID: PMC8716672. |
| [7] | Akhan O., Erdoğan E., Ciftci T.T., Unal E., Karaağaoğlu E., Akinci D. Comparison of the Long-Term Results of Puncture, Aspiration, Injection and Re-aspiration (PAIR) and Catheterization Techniques for the Percutaneous Treatment of CE1 and CE3a Liver Hydatid Cysts: A Prospective Randomized Trial. Cardiovascular and Interventional Radiology. 2020; 43(7): 1034-1040. doi: 10.1007/s00270-020-02477-7. |
| [8] | Brunetti E, Kern P, Vuitton DA; Writing Panel for the WHO-IWGE. Expert consensus for the diagnosis and treatment of cystic and alveolar echinococcosis in humans. ActaTrop. 2010 Apr; 114 [1]: 1-16. doi: 10.1016/j.actatropica.2009.11.001. Epub 2009 Nov 30. PMID: 19931502. |
| [9] | Brunetti E, Maiocchi L, Garlaschelli AL, Gulizia R, Filice C. Attualità in tema di terapiadell' echinoccocosi cistica. Parassitologia. 2004 Jun; 46 [1-2]: 53-5. Italian. PMID: 15305686. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML