-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(1): 30-32
doi:10.5923/j.ajmms.20261601.08
Received: Dec. 18, 2025; Accepted: Jan. 2, 2026; Published: Jan. 7, 2026

Modern Aspects of Genital Prolapse Treatment
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKurbanov D. D. , Khamdamova S. A.
Tashkent State Medical University, Uzbekistan
Correspondence to: Kurbanov D. D. , Tashkent State Medical University, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

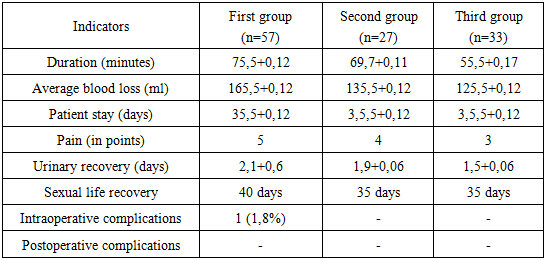
Prolapse of female genital organs is one of the acute problems of modern gynecology. Objective of the study: To conduct a differentiated approach to surgical treatment of genital prolapse in women, depending on the degree of prolapse, the age of women and the state of reproductive health. Materials and methods of the study: 57 operations of hysterectomy by vaginal access using a new technology with strengthening of the ligamentous apparatus and fixation of the vaginal stump using synthetic prolene tape, 27 operations of sacropexy in combination with anterior and posterior colpoperineolevatorplasty, 33 operations for correction of genital prolapse in combination with plication of the uterine-keratotic ligaments and anterior posterior colpoperineolevatorplasty were performed. Results of the study: The choice of technique was carried out depending on the size of the uterus, its mobility, features of its location, vaginal capacity, previous operations. If necessary, appendages were removed, adhesions were eliminated. The size of the uterus reached values corresponding to 22 weeks, and on average 15 weeks of pregnancy, depending on the concomitant disease. Conclusions: In women with grade I genital prolapse of reproductive age who wish to preserve generative function, shortening of the sacrouterine ligaments using synthetic prolene tape has been found to be highly effective.
Keywords: Prolapse, Hysterectomy, Sacropexy
Cite this paper: Kurbanov D. D. , Khamdamova S. A. , Modern Aspects of Genital Prolapse Treatment, American Journal of Medicine and Medical Sciences, Vol. 16 No. 1, 2026, pp. 30-32. doi: 10.5923/j.ajmms.20261601.08.
1. Relevance
- Treatment methods for women with genital prolapse vary dramatically depending on the woman's age, prolapse severity, complaints, and medical history. The choice of treatment method increasingly remains a mystery. There is no consensus on the choice of surgical approach, the use of mesh products or allografts, and some gynecologists resort to conservative treatment methods altogether. [1,3].Surgical treatment of genital prolapse has always remained a priority, as it is the only method for completely eliminating the disease. However, surgical interventions still leave numerous complications, both intra- and postoperative. [4,7]. Furthermore, the prevention of complications is also controversial.Today, the key issue is the choice of surgical treatment method based on the following factors: prolapse severity, complaints and age of the woman, sexual activity, and reproductive health.Also, when determining surgical treatment tactics, it is necessary to carefully differentiate between the various types of prolapse and prevent long-term complications and recurrences. [5,9].There are numerous studies examining the effectiveness of various treatments for genital prolapse, depending on the severity of the lesion and the age of the patient. These studies include cohort, randomized, and placebo-controlled trials. The risk of prolapse recurrence, vaginal stump prolapse, postoperative fistula formation, and stress urinary incontinence remains unpredictable. None of the existing surgeries provides clear assurance of preventing the above complications. [3]. Study Objective: To conduct a differentiated analysis of the results of surgical correction of genital prolapse in women, based on the intraoperative and postoperative findings.
2. Research Methods
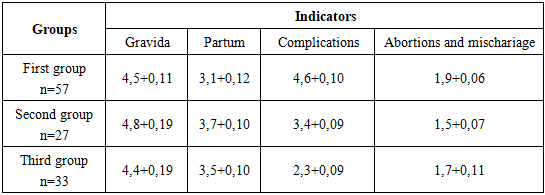
- We analyzed the medical records of 117 women (retrospectively) from 2020-2025. We studied women with varying degrees of genital prolapse admitted for elective surgery at Tashkent City Interdistrict Perinatal Center No. 6. We divided the women into three groups: The first group consisted of 57 women with severe genital prolapse, operated on using our proprietary technique (patent IAP 2020 0279). The second group consisted of 27 women with moderate to mild prolapse who underwent sacropexy. The third group consisted of 33 women with predominantly posterior vaginal wall prolapse, who underwent uteruterosacral ligament suspension and colpoperineolevatorplasty.The women examined ranged in age from 37 to 76 years. The diagnosis of genital prolapse was established based on the patient's medical history and laboratory and instrumental examination data (according to the POP 2020 classification). All women admitted to inpatient treatment underwent a standard comprehensive examination. The surgical treatment method was selected individually based on the location of the hernial orifice, vaginal length, the condition of the ligamentous apparatus, and the woman's wishes.
3. Results
- We carefully reviewed the women's medical histories. We conducted a comprehensive assessment of their reproductive, gynecological, and obstetric histories. All data were entered anonymously. A significant obstetric history, as well as complications during childbirth, were noteworthy. As can be seen from the first table, most women were multiparous, had delivered large fetuses, and had multiple cervical, vaginal, and perineal lacerations. Possibly, an aggravated obstetric history is the leading cause of the development of genital prolapse, which is also confirmed by literary sources.
|
|
4. Conclusions
- 1. Our analysis showed that for older and elderly women without the need for restoration of reproductive function, surgery using our technique is the preferred option. 2. For women with mild genital prolapse and potential reproductive potential, pelvic floor strengthening by suspending the uterosacral ligaments has been shown to be highly effective. 3. For women with grades II-III genital prolapse, sacropexy is recommended.