-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(12): 4635-4639
doi:10.5923/j.ajmms.20251512.97
Received: Nov. 28, 2025; Accepted: Dec. 15, 2025; Published: Dec. 26, 2025

Specific Characteristics of Standard and Complex Orthodontics Treatment in Early Children with Anomalies in the Tooth-Jaw System
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLEshonqulov Golibjon Turaqulovich
Bukhara State Medical Institute named after Abu Ali Ibn Sino, Bukhara, Uzbekistan
Correspondence to: Eshonqulov Golibjon Turaqulovich, Bukhara State Medical Institute named after Abu Ali Ibn Sino, Bukhara, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Currently, the prevalence of dental jaw anomalies in orthodontic dental practice is higher than 50%, according to the World Health Organization as a whole. According to scientific research work, the rate of incidence of dental jaw abnormalities in children's age in our country is 48 - 62 %. sucks. The age related prevalence of dental-jaw abnormalities in early school age is most common among children between the ages of 3 and 6, and between the ages of 7 and 9 at school age. Among children of early school age and school age, early detection of dental jaw anomalies, study of prevalence indicators, development of effective treatment methods and implementation in practice are some of the pressing problems.
Keywords: Dental-jaw abnormalities, Children of early school age and school age, Early diagnosis of dental-jawomas and complex treatment methods
Cite this paper: Eshonqulov Golibjon Turaqulovich, Specific Characteristics of Standard and Complex Orthodontics Treatment in Early Children with Anomalies in the Tooth-Jaw System, American Journal of Medicine and Medical Sciences, Vol. 15 No. 12, 2025, pp. 4635-4639. doi: 10.5923/j.ajmms.20251512.97.
1. Introduction
- Effective work has been carried out among children of early school age and school age to develop methods of early diagnosis and complex treatment of dental-jawomalia, to obtain a stable aesthetic result in the treatment of orthodontic sick children, and to reduce the number of relapses. Nevertheless, existing methods of diagnosis are insufficient, creating a strong need for further methods of diagnosis and treatment. In this respect, the development of diagnostic and therapeutic measures aimed at increasing the quality indicators of orthodontic care in children of early school age and school age is becoming important in the practice of orthodontic dentistry. Today in our country, great work is being carried out on providing medical care to the population in the health system, its organization, including the radical improvement of the provision of orthodontic care in children of early school age and school age, the early diagnosis of Maxillofacial diseases in children and the Prevention of its transition to uncomplicated deformities. The field of orthodontics began to gain significant importance in dentistry, and this trend continues today. Modern research into long-lasting efficacy in orthodontic treatment has found that many of those who undergo orthodontic treatment courses are satisfied with the results of the treatment and have seen its positive benefits. All patients, to an astonishing extent, felt dental and facial models, but almost all recognize that along with the condition of the teeth, psychological status has improved. In the last decades, many new methods and means of treatment have appeared in the field of orthodontics, which allow the orthodontist to carry out the necessary treatment and preventive measures in the early stages of the formation of the disease. However, even today, when correcting tooth-jaw disorders and deformities, while not allowing optimal results in terms of duration and quality of treatment, traditional methods have not lost their effectiveness. In assessing the effectiveness of the orthodontic treatment carried out, the following can serve as a criterion: its duration, standards of orthodontic methods and the results obtained on its stability. To carry out an effective orthodontic treatment course, it must be carefully planned. In mixed bites, orthodontic treatment is often carried out. In the case of problems of the average difficulty stage during the mixed bite period, treatment may be sufficient in eliminating all anomalies and may be carried out by a doctor-dentist in general practice. Treatment of children with serious problems is carried out in two stages: the first – during the period of mixed bites, the second – during the period of early bites on permanent teeth. Such treatment usually requires the participation of a specialist [2,4,6,8,10,12,14].
2. Results and Analyzes
- If more than six months remain until the rupture of permanent premolars, it will be extremely important to maintain a place in the tooth row in the absence of the first or second temporary molar. Otherwise the area may remain closed until the premolars burst. The potential deficit of the place can be caused by the loss of teeth before the time, or by the passive displacement of permanent curled teeth or molars through the initial rupture of permanent molars. In children with an intermediate degree of anomaly (i.e., without skeletal changes), the Lost range can be restored by moving and changing the location of the teeth. After that, it is recommended to wear a device that will keep that intermediate place until permanent teeth crack. In the case of shortening the umuic length of the tooth row without early loss of milk teeth, a permanent cranial tooth position is observed. Aesthetics is the main advantage in the treatment of this deformity during the mixed bite period. Such treatment measures are often carried out with the desire of their parents than children. If the upper curled teeth are bent forward and the lower curled teeth do not touch each other, the protrusion of the upper curled teeth can be eliminated by slanting them using a simple device. This condition can be caused by sucking the big toe during the mixed bite period and is associated with a narrowing of the upper tooth row. Physiological adaptation in the presence of Sagittal suture is the placement of the tongue between the teeth in the process of speech and swallowing. A diastema between the teeth of the upper central cranium can present a special problem in itself. In the absence of a deep shovel tooth covering, such slits usually close on their own. However, when the upper central cranial tooth spacing is more than 2 mm, it does not close on its own. The distance maintained between the cranial teeth is related to the alveolar new tooth interval between the central cranial teeth, in which the upper lip-holding wedge is located. When correcting large-sized diastems, the retaining fibers will need to be surgically removed. In children, transverse occlusion during the period of a crossed bite occurs as a result of narrowing of the upper tooth row. If in this case the intervention of the lower jaw is observed when closing the mouth, the correction of the anomaly should be started earlier. Otherwise, treatment can be postponed for several periods, especially when there are other abnormalities that require correction at a later age. In a child with good-looking facial proportions, vertical shovel tooth dysocclusion is limited to the area of the front teeth. The main cause of this anomaly is sucking the big toe, and the main step in correcting will be the removal of a harmful habit. This requires a special changed form of the child's character and an instruction that blocks this harmful habit [1,3,5,7,9,11,13,15].The purpose of the study is to detect the spread of dental-jaw anomalies in children's age, as well as to improve effective treatment on a par with early age-related diagnosis. Object of study. The scientific work was based on the results of research carried out during 2019-2021 in 1,066 sick children under the supervision of a dentist-orthodontist in Bukhara region Karakul, Olot, Gijduvan districts and Bukhara city children's dental clinics. The subject of the study was: Anamnesis data collected from patients and their parents who have dental –jaw abnormalities of early school age and school age. Research methods. The study used clinical, dental, anthropometric, radiological, orthopantomogram, functional and statistical analysis. As we know, parents often complain to the orthodontist reception of a cosmetic defect on the face of the child's jaw. In orthodontic problems, there are often cases when the child does not have complaints, and after it manifests itself in many cases with a violation of aesthetic appearance, there are cases when permanent teeth do not come out in time, or do not come out at all. The patient often has time to avoid permanent tooth dislocation in the jaw or when the tooth comes out of the arc row at the edge and has to give up permanent teeth to correct it. In orthodontic practice, the tactic of removing permanent teeth, such as the first or second permanent premolar, is heavily used to correct the defect. In some cases, the affected teeth are removed using rigid orthodontic tools and pulled into an orthodontic knob mounted on the most convenient surface of the crown, which is surgically open.Based on the tasks of the research work, age – related treatment measures for children in comparative groups were carried out as follows: sharpening teeth without physiological suction in children 3-6 years old, jarring existing short arches under the lip and tongue, installing removable devices to prevent tooth displacement if milk teeth were removed earlier than the deadline, and traditional treatment measures based on the According to him, we applied the prostheses with a plate to take milk teeth and prophylactically remove. Short grooves, which occur as a congenital anomaly in early children, interfere with the normal growth of the lower and upper jaw, disrupting the dynamic position of the teeth, leading to dental diastema, speech disorders and subsequent bite Disorders, pathological biting. Also, in these young gurukhs, conversations were held with the parents of children with harmful habits, we sent to the children's neurologist, speech therapist and other relevant specialists.
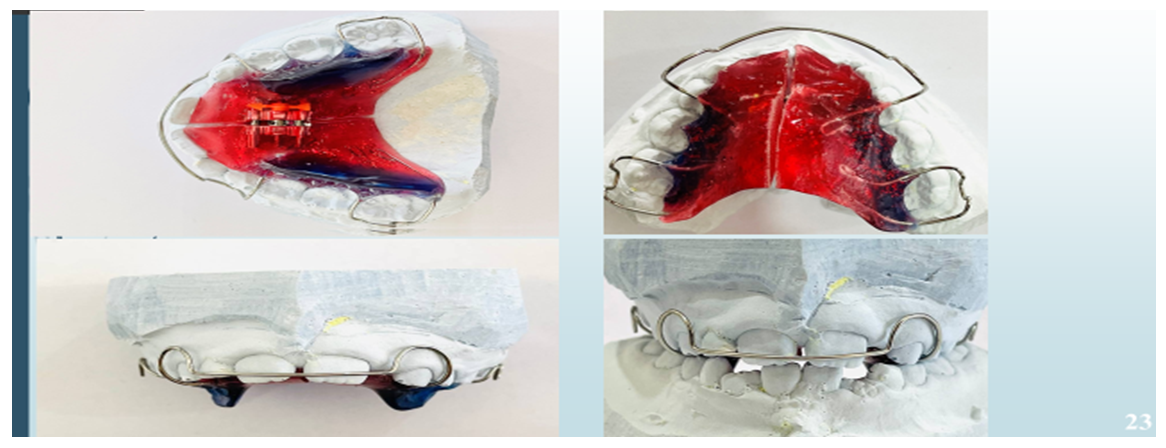 | Figure 1. Laboratory-fabricated removable orthodontic appliances and their fitting on plaster models, designed to manage space deficiency and guide the eruption of permanent teeth |
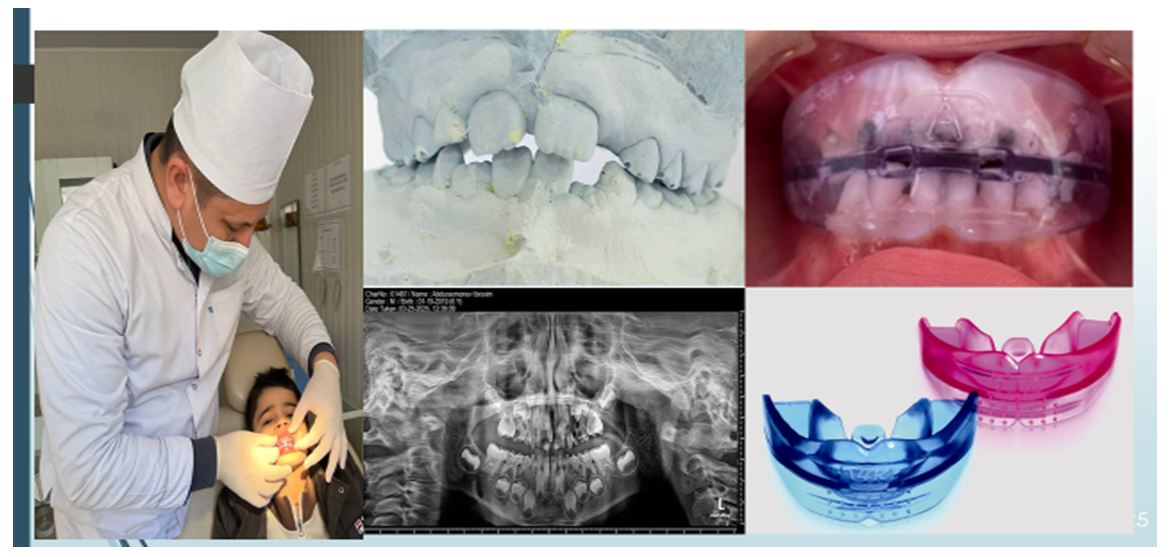 | Figure 2. Clinical, radiographic, and laboratory findings in a patient with insufficient arch space during mixed dentition, including intraoral examination, plaster diagnostic models, panoramic radiograph, and removable orthodontic appliances |
 | Figure 3. Clinical application and laboratory fabrication stages of the orthodontic appliance used to modify the direction of tooth eruption and extraction in children during the mixed dentition period |
3. Conclusions
- The results obtained after complex orthodontic treatment showed that all children who were in the early mixed bite period, that is, who applied in the early period of age 7-9 years, and received comprehensive therapeutic and preventive dental care for a year, showed a decrease in initial gross violations in the gums.