-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(12): 4605-4609
doi:10.5923/j.ajmms.20251512.90
Received: Oct. 15, 2025; Accepted: Nov. 12, 2025; Published: Dec. 25, 2025

Improving Rehabilitation for Children with Moderate Sensorineural Hearing Loss
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLFattakhova Nargizakhon Mirzokhidovna
Tashkent Medical Academy, Tashkent, Republic of Uzbekistan
Correspondence to: Fattakhova Nargizakhon Mirzokhidovna, Tashkent Medical Academy, Tashkent, Republic of Uzbekistan.
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Moderate sensorineural hearing loss in children represents a significant challenge for both clinical practice and educational development. Timely diagnosis and effective rehabilitation programs are crucial to prevent delays in speech, cognitive, and social skills. This article examines current approaches to pediatric auditory rehabilitation, highlighting the role of modern hearing technologies, individualized therapy, and interdisciplinary collaboration. Special attention is given to optimizing rehabilitation strategies that integrate medical, psychological, and pedagogical support. By improving early intervention and tailoring treatment plans to the specific needs of each child, rehabilitation outcomes can be significantly enhanced, contributing to better communication skills and overall quality of life.
Keywords: Sensorineural hearing loss, Pediatric rehabilitation, Auditory therapy, Early intervention, Individualized approach
Cite this paper: Fattakhova Nargizakhon Mirzokhidovna, Improving Rehabilitation for Children with Moderate Sensorineural Hearing Loss, American Journal of Medicine and Medical Sciences, Vol. 15 No. 12, 2025, pp. 4605-4609. doi: 10.5923/j.ajmms.20251512.90.
Article Outline
- Sensorineural hearing loss (SNHL) is a persistent impairment of auditory function resulting from damage to the inner ear structures, the auditory nerve, or the central pathways of the auditory system. In children, this condition is of particular concern, since hearing is essential for the development of speech, cognitive processes, and successful social integration [1]. According to the World Health Organization, more than 34 million children worldwide are affected by hearing loss, and over 60% of these cases could be prevented or effectively managed with timely intervention [2].Recent years have seen a growing number of cases of SNHL identified in early childhood. This alarming trend is linked to multiple factors, including environmental deterioration, the rising incidence of perinatal pathologies, intrauterine infections, hereditary diseases, and the insufficient level of prenatal diagnostics in certain regions [3]. Among the various forms of hearing loss, moderate sensorineural hearing loss (41–55 dB reduction) is particularly insidious, as it often goes unnoticed for an extended period, especially if the child has not yet begun to speak actively. The lack of early detection and intervention contributes to secondary delays in speech and intellectual development, reduced learning capacity, and, later in life, significant social and professional limitations [4].In this context, one of the primary challenges of modern pediatric otorhinolaryngology, speech therapy, and special education is the improvement of rehabilitation strategies for children with moderate SNHL. The development and implementation of individualized auditory-verbal rehabilitation programs aimed at early and comprehensive restoration of auditory function and speech are crucial. However, despite the availability of standardized clinical protocols, the effectiveness of many rehabilitation programs remains insufficient. This is largely due to delayed diagnosis and the lack of a systemic approach that considers the child’s age, neurological status, and psycho-emotional characteristics [5] [6].Modern research demonstrates that the best outcomes are achieved through a multidisciplinary approach, involving collaboration among otorhinolaryngologists, audiologists, speech therapists, neurologists, and child psychologists. Such coordinated efforts make it possible not only to restore auditory perception but also to ensure the development of intelligible speech, successful socialization, and an improved quality of life for the child [7].Therefore, the need to enhance the effectiveness of auditory-verbal rehabilitation for children with moderate sensorineural hearing loss has become an essential priority in both clinical practice and scientific research.
1. Participants and Study Design
- The study was conducted at the Department of Otorhinolaryngology of the Tashkent Medical Academy between 2022 and 2024. A total of 80 children aged 3 to 7 years with a confirmed diagnosis of moderate sensorineural hearing loss (Grade II, 41–55 dB) were enrolled. The participants were divided into two groups of 40 children each: the main group (Group I) and the control group (Group II). Allocation was carried out with consideration of age, sex, degree of hearing loss, and the presence of concomitant somatic disorders.
2. Rehabilitation Program
- Children in the main group received a comprehensive auditory-verbal rehabilitation program, which included:individualized selection and fitting of digital hearing aids;regular sessions with a speech therapist-defectologist (at least three times per week);auditory training based on specialized acoustic stimulation;psycho-emotional support involving both a child psychologist and parental counseling;continuous medical supervision (pediatrician, neurologist, and otorhinolaryngologist).The control group underwent standard therapy, which consisted only of hearing aid fitting and occasional speech therapy sessions (no more than once per week).
3. Assessment Methods
- To evaluate the effectiveness of rehabilitation, the following methods were applied:Audiological diagnostics: pure-tone threshold audiometry with determination of auditory thresholds before and after intervention.Speech and language testing: assessment of phonemic awareness, active and passive vocabulary, and connected speech.Cognitive and social adaptation: evaluation of memory, attention, and social adaptation in a peer group using the “SocD” social behavior scale.Parental perception: questionnaires measuring satisfaction with rehabilitation outcomes.Dynamic monitoring: intermediate control points were established at baseline (T0), after 6 months (T1), and after 12 months (T2).Statistical AnalysisAll data were recorded in individual observation charts and analyzed using descriptive statistics. Comparisons between groups were conducted using Student’s t-test. A significance level of p < 0.05 was considered statistically significant.
4. Results
- Children in the main group demonstrated significant progress across all evaluated parameters. The average hearing threshold improved from 50.2 dB to 37.1 dB (p < 0.01). Active vocabulary increased by approximately 1.5 times, and improvements were observed in pronunciation as well as grammatical speech structure. In contrast, changes in the control group were less pronounced and statistically insignificant.Social adaptation in a peer group improved in 87% of children in the main group, compared to 58% in the control group. Parental satisfaction with rehabilitation quality was also higher in the main group (91% vs. 63%).After 12 months of observation of children with Grade II sensorineural hearing loss in both groups, a pronounced positive dynamic was recorded in auditory perception, speech development, and social adaptation among those who underwent comprehensive individualized rehabilitation.A particularly illustrative parameter was the Basic Hearing Scale (BHS), which characterizes the perception of speech and background sounds. In the main group (Group I), the mean baseline value was 15.9 points. After 6 months (T1), this improved to 17.5, and by the end of 12 months (T2), it reached 19.0, corresponding to a total increase of +3.1 points. In the control group (Group II), the baseline value was 14.9, increasing to 15.7 at 6 months and 16.8 at 12 months, showing only a +1.9-point improvement. The difference between the groups at the final stage was statistically significant (p < 0.05).
 | Figure 1. Dynamics of auditory perception (Basic Hearing Scale, BHS) at three stages of observation: baseline (T0), after 6 months (T1), and after 12 months (T2) |
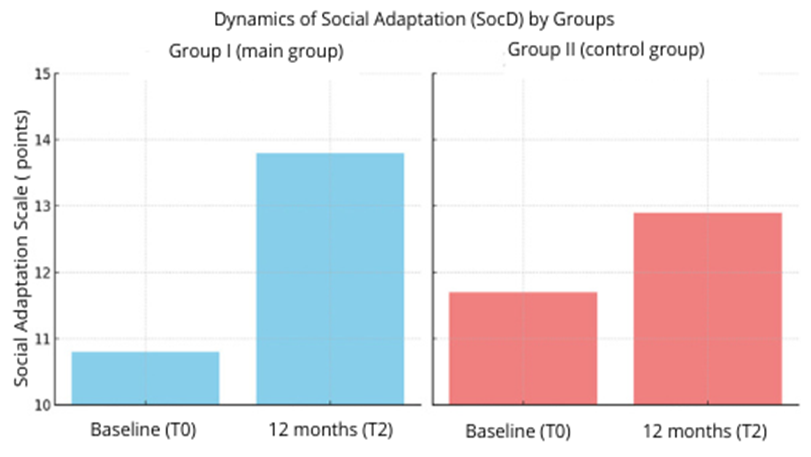 | Figure 2. Dynamics of social adaptation (SocD) in children of the main and control groups over 12 months |
|

|

5. Discussion
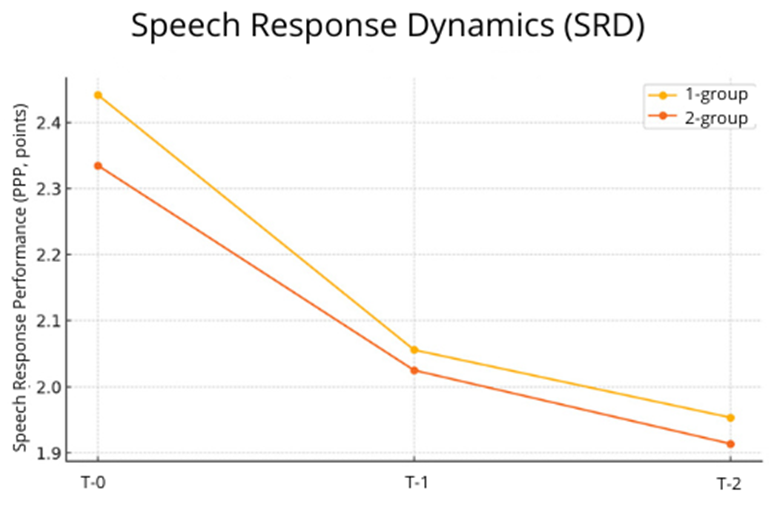
- The results of this study confirm the high effectiveness of comprehensive auditory-verbal rehabilitation in children with moderate sensorineural hearing loss. Children in the main group demonstrated significant improvements in auditory, speech, and social skills compared to those in the control group who received standard therapy. These findings are consistent with the results of similar studies that emphasize the advantages of a multidisciplinary approach [1] [4] [5].The most distinct difference was observed in auditory perception dynamics: over 12 months, the Basic Hearing Scale (BHS) in the main group increased by an average of 3.1 points, whereas in the control group the improvement was only 1.9 points. This highlights the importance of individualized hearing aid adjustment and regular auditory training aimed at developing auditory perception and phonemic awareness [2] [6].Speech development also showed statistically significant improvement in the main group. A reduction of the Speech Response Rating (SRR) by 0.5 points during the year reflects the formation of more stable speech skills, vocabulary expansion, and the ability to construct connected speech. In the control group, changes were minimal, likely due to the insufficient intensity of speech therapy sessions.Particular attention should be given to the social adaptation parameter (SocD), which improved by +3.0 points in the main group, as clearly demonstrated by the diagrams. Enhancements in this area can be attributed to the involvement of a child psychologist in the rehabilitation program and parental training in interaction strategies with hearing-impaired children. Social inclusion, emotional intelligence, and communication skills proved to be highly responsive to psycho-emotional support, which is consistent with findings from other studies in this field [3][7].Thus, the results of this study not only confirm the relevance of implementing a comprehensive rehabilitation model, but also emphasize the necessity of adapting it to the individual characteristics of each child. Such an approach makes it possible not only to compensate for hearing deficits but also to prevent secondary complications related to emotional well-being, learning ability, and social integration.
6. Conclusions
- Based on the clinical study conducted, the following conclusions can be drawn:Comprehensive auditory-verbal rehabilitation with an individualized approach—including modern digital hearing aids, regular speech therapy sessions, auditory training, and psychosocial support—proved to be more effective than the standard scheme of care for children with moderate sensorineural hearing loss.Children in the main group demonstrated significant improvement in auditory perception (+3.1 points), speech development (SRR reduction by –0.5 points), and social adaptation (+3.0 points), whereas progress in the control group was significantly lower.The introduction of multimodal rehabilitation methods into pediatric otorhinolaryngology and speech therapy practice substantially improves the quality of life of children with hearing loss, supports their successful social integration, and fosters the development of a well-rounded personality.The results highlight the necessity of early initiation of rehabilitation (preferably before the age of 4), interdisciplinary collaboration among specialists, and active parental involvement in the restoration of auditory-verbal functions.The presented program can be recommended for broad implementation in audiology and speech therapy centers, and also as a model for adaptation in public healthcare institutions engaged in the rehabilitation of children with hearing impairments.