Dilbar S. Tuksanova1, Feruza S. Khudoykulova2
1PhD Student of the Department Gynecology-2 and Obstetrics at Bukhara State Medical Institute, Bukhara, Uzbekistan
2DSc, Professor, Head of the Department Gynecology and Obstetrics-2 at Bukhara State Medical Institute, Bukhara, Uzbekistan
Correspondence to: Dilbar S. Tuksanova, PhD Student of the Department Gynecology-2 and Obstetrics at Bukhara State Medical Institute, Bukhara, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Preeclampsia is a multisystem hypertensive disorder of pregnancy characterized by progressive endothelial dysfunction and hemodynamic instability, often accompanied by neurological complications. This study evaluated the correlation features between systemic hemodynamic parameters and brain MRI indicators in pregnant women with preeclampsia of varying severity. Analysis demonstrated that severe preeclampsia is associated with marked alterations in cerebral perfusion and vascular reactivity, correlating with abnormal biochemical markers and elevated blood pressure. MRI revealed symmetrical hyperintense foci in the occipito-parietal regions consistent with vasogenic edema, typical of posterior reversible encephalopathy syndrome (PRES). These neuroimaging changes reflect systemic endothelial injury and hypertensive CNS involvement. Importantly, follow-up imaging showed full regression of abnormalities after blood pressure stabilization and delivery, confirming the reversible nature of cerebral dysfunction. The combined assessment of hemodynamic, biochemical, and MRI parameters enhances early detection of target-organ involvement and provides a reliable framework for predicting disease severity and guiding timely management in preeclamptic pregnancies.
Keywords:
Preeclampsia, Hemodynamics, MRI, PRES, Endothelial dysfunction, Cerebral perfusion, Pregnancy hypertension, Reversible encephalopathy, Maternal health
Cite this paper: Dilbar S. Tuksanova, Feruza S. Khudoykulova, Evaluation of Correlation Features of Hemodynamic Parameters with MRI Indicators in Pregnant Women with Preeclampsia, American Journal of Medicine and Medical Sciences, Vol. 15 No. 12, 2025, pp. 4594-4597. doi: 10.5923/j.ajmms.20251512.87.
1. Introduction
Preeclampsia (PE) is a multifactorial complication of pregnancy, the etiology and pathogenesis of which remain the subject of intensive study. Current understanding is based on the concept of systemic endothelial dysfunction resulting from impaired placentation, an imbalance of angiogenic factors, oxidative stress, and immune and genetic mechanisms [1].Posterior reversible encephalopathy syndrome (PRES) is a pathological condition characterized by vasogenic edema and disruption of the blood-brain barrier (BBB), affecting both the cortical and subcortical regions of the brain, including various anatomical areas [2,3]. Most often, the pathological process is localized in the parieto-occipital zones, often accompanied by visual impairment or temporary cortical blindness. In severe clinical cases, PRES can lead to coma, status epilepticus, and intracranial hemorrhage. Similar changes can also occur outside of pregnancy, for example, in patients with acute hypertension, chronic kidney disease, or the use of immunosuppressive drugs such as calcineurin inhibitors [4,5]. Radiological signs of PRES are found in nearly 98% of women with eclampsia, leading to debate among specialists about whether eclampsia can be considered a specific variant of "obstetric PRES." However, it is known that PRES developing in the context of preeclampsia has its own distinctive features: it is more often accompanied by severe headaches, is less likely to present with cognitive impairment, and likely has a more favorable course [6].The aim of the study was to conduct a correlation analysis of blood hemodynamic parameters and brain MRI parameters in pregnant women with preeclampsia.
2. Materials and Methods
In accordance with the goals and objectives of the study, 90 women will be examined. The research program will be implemented at the Bukhara Regional Branch of the Republican Specialized Scientific and Practical Medical Center for Maternal and Child Health in collaboration with the Department of Obstetrics and Gynecology No. 2 of the Bukhara State Medical Institute. Standard laboratory and instrumental diagnostic methods and hemocoagulation systems (fibrinogen, platelets, PI, APTT, D-dimer), clinical and biochemical tests (CRP, complete blood count, urine analysis), Doppler ultrasound of the carotid arteries, and functional MRI will be used. In-depth studies were conducted on a contingent of 90 women, including 30 patients with a physiological course of pregnancy and childbirth (1 control group), the main prospective group consisted of 60 patients, of which 30 patients were registered at the end of the second trimester of pregnancy, who did not receive appropriate preventive therapy (2 group) and 3 group consisted of patients registered from the early stages of pregnancy and promptly underwent a comprehensive examination and received therapy aimed at preventing hypoxic-ischemic brain damage.Maternal serum samples are used to study key biochemical and hemostatic parameters. Central hemodynamics and cerebral blood flow are determined using Doppler ultrasound. Structural brain abnormalities are assessed using MRI. Statistical methods are used to process the data and analyze treatment results. Furthermore, patients' quality of life is assessed using standardized questionnaires to evaluate the effectiveness and safety of transcatheter interventions.
3. Results
To objectively characterize brain damage in pregnant women with severe preeclampsia, magnetic resonance imaging (MRI) was performed using FSE_T2_FLAIR, T1_FLAIR, and DWI modes. The study was performed on axial, coronal, and sagittal sections with a 5-mm slice thickness.Brain MRIs (Figs. 1, 2) reveal areas of hyperintensity on FLAIR sequences, predominantly in the occipito-parietal regions of the white matter, with a tendency toward symmetrical distribution. These changes are characterized by vasogenic edema without signs of mass effect, midline displacement, hemorrhage, or ischemic injury.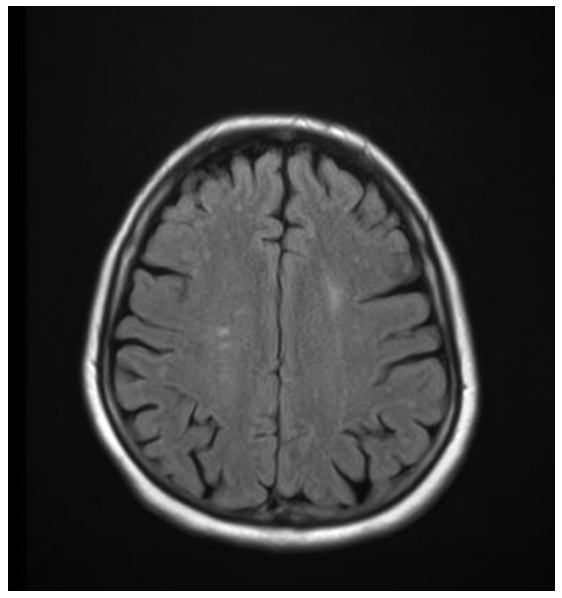 | Figure 1. MRI of the brain of patient Z.T., with severe preeclampsia (axial slice, FSE_T2_FLAIR mode): hyperintense foci of vasogenic edema in the occipital-parietal regions |
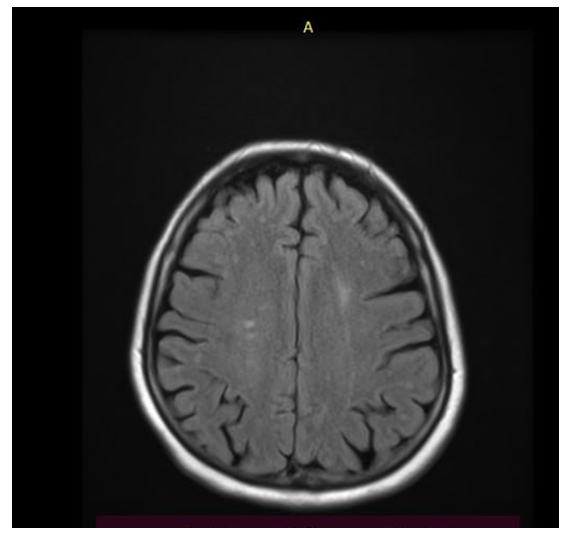 | Figure 2. MRI of the brain of the same patient: symmetrical areas of increased signal on FLAIR, characteristic of posterior reversible encephalopathy syndrome (PRES) |
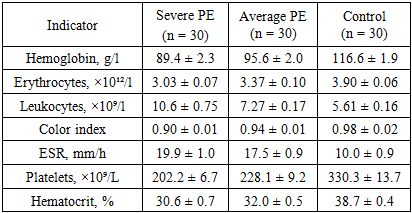
The ventricular system is not dilated, the contours are clear, and the subarachnoid spaces are not deformed. On FSE_T2 and T1 FLAIR sections, the structure of the corpus callosum and brainstem is preserved, and no signs of focal necrotic changes are detected. Dynamic observation 10-14 days after delivery showed regression of foci of hyperintensity, confirming the reversible nature of the process.The obtained data indicate the presence of typical MRI signs of reversible posterior encephalopathy syndrome (Posterior Reversible Encephalopathy Preeclampsia Retinopathy Syndrome (PRES) occurs in patients with severe preeclampsia. This syndrome develops as a result of hypertensive crisis, endothelial dysfunction, and impaired cerebral blood flow autoregulation, leading to increased permeability of the blood-brain barrier and the development of vasogenic edema.Visualized areas of hyperintensity in the white matter of the parieto-occipital lobes reflect reversible perfusion disturbances. The absence of signs of cytotoxic edema and necrosis confirms the benign nature of the process, provided blood pressure is corrected promptly and delivery is performed.Correlation analysis showed a significant relationship between the severity of hyperintensive changes and hemodynamic parameters (r = 0.62; p < 0.01) and coagulation status (r = 0.58; p < 0.05), which reflects the systemic nature of vascular disorders in severe preeclampsia.Table 1 presents the data of the general blood test in pregnant women with severe (group 1a) and moderate (group 1b) preeclampsia compared to the control group.Table 1. Main indicators of general blood analysis in examined pregnant women (M ± m)
 |
| |
|
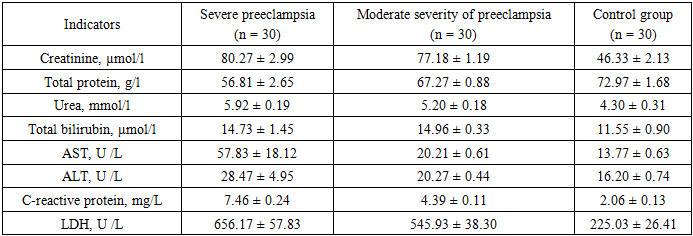
In patients with severe preeclampsia, a statistically significant decrease in hemoglobin levels (89.4 ± 2.3 g/l; p < 0.001) and red blood cell counts (3.03 ± 0.07 × 10¹²/l; p < 0.01) was observed compared with the control group, indicating the development of hemodilution and anemic syndrome against the background of systemic hyperhydration and vascular dysfunction.The number of leukocytes in this group reached 10.6 ± 0.75 × 10⁹/l, which exceeds the values in the control group by almost 1.9 times (p < 0.001), reflecting the activation of the systemic inflammatory response characteristic of endothelial dysfunction in preeclampsia.The color index in most of the examined subjects remained within the normal range (0.90–0.98), which excludes iron deficiency anemia, confirming the hemodilution mechanism.The erythrocyte sedimentation rate (ESR) increased significantly in the severe form—by 1.9 times compared to the control (19.9 ± 1.0 mm/h versus 10.0 ± 0.9 mm/h; p < 0.01). This indicates the presence of inflammatory syndrome and hyperfibrinogenemia.Platelet counts showed a significant downward trend in pregnant women with severe preeclampsia (202 ± 6.7 × 10⁹/L), which may reflect the early stages of DIC and activation of the coagulation cascade. In the moderate group, platelet counts remained at 228 ± 9.2 × 10⁹/L but remained lower than those in the control group (p < 0.05).Hematocrit also showed a decrease (30.6 ± 0.7% in severe and 32.0 ± 0.5% in moderate form versus 38.7 ± 0.4% in the control; p < 0.01), which is associated with an expansion of plasma volume and relative anemia.The data obtained reflect an increase in inflammatory and hemocoagulation disorders and severe hemodilution as preeclampsia worsens. Taken together, these changes indicate progressive endothelial damage, activation of the blood coagulation system, and systemic tissue hypoxia.Such abnormalities correlate with increased CRP and fibrinogen levels, as well as with MRI-detected signs of cerebral edema and reversible encephalopathy, which will be discussed in detail in subsequent sections.The data presented demonstrate that pregnant women with severe preeclampsia, compared with the control group, exhibited a significant (p < 0.001) increase in creatinine, urea, and cytolytic enzymes (AST, ALT, LDH), reflecting liver dysfunction and cellular distress. Total protein concentration in this group was significantly reduced (56.8 ± 2.6 g/L versus 72.9 ± 1.7 g/L in the control group), indicating the development of hypoproteinemia and increased vascular permeability syndrome.C-reactive protein levels in pregnant women with severe preeclampsia were 3.6 times higher than control values, confirming a pronounced systemic inflammatory response. LDH, an enzyme reflecting tissue hypoxia, increased more than 2.9 times compared to normal, correlating with clinical signs of hypoperfusion and MRI data.In moderate preeclampsia, the changes were intermediate: an increase in LDH and C-reactive protein was combined with a moderate increase in AST and ALT and a partial decrease in plasma protein.When analyzing the biochemical blood parameters (Table 2), significant differences were revealed between the groups of pregnant women with severe and moderate preeclampsia compared to the control group. In patients with a severe form of the disease, a significant increase in creatinine levels was observed to 80.3 ± 2.9 μmol/l versus 46.3 ± 2.1 μmol/l in the control (p < 0.001), indicating impaired glomerular filtration and the development of nephropathic syndrome. A moderate increase in urea concentration (5.92 ± 0.19 mmol/l) in severe preeclampsia also confirms kidney involvement in the pathological process and correlates with an increase in C-reactive protein levels (r = 0.61, p < 0.01).Table 2. Blood biochemical analysis parameters in pregnant women with preeclampsia of varying severity and in the control group (M ± m)
 |
| |
|
The total protein level in this category of patients was significantly reduced (56.8 ± 2.6 g/L versus 72.9 ± 1.6 g/L in the control, p < 0.01), reflecting hypoproteinemia resulting from increased vascular permeability, urinary protein loss, and activation of the inflammatory response. In the moderate-severity group, the protein level was 67.3 ± 0.9 g/L, which was also lower than the control values, but the difference was less pronounced (p < 0.05).Bilirubin in patients with severe preeclampsia reached 14.7 ± 1.5 μmol/L, while in the control group this indicator was 11.5 ± 0.9 μmol/L, indicating the initial signs of cytolysis and possible liver involvement in the pathological process. Elevated levels of liver enzymes - AST (57.8 ± 18.1 U /L) and ALT (28.5 ± 4.9 U /L) - indicate the development of cytolysis syndrome and hypoxic damage to hepatocytes. In the moderate group, these enzymes had lower values (AST = 20.2 ± 0.6 U /L, ALT = 20.3 ± 0.4 U /L), indicating a lesser degree of liver dysfunction, corresponding to a more favorable course of the disease.Of particular importance is the C-reactive protein level, which in pregnant women with severe preeclampsia was 7.46 ± 0.24 mg/L, which is 3.6 times higher than the control group (2.06 ± 0.13 mg/L, p < 0.001). This reflects a pronounced inflammatory response and endothelial activation. In patients with moderate preeclampsia, the CRP value was moderately elevated—4.39 ± 0.10 mg/L, which is consistent with the clinical manifestations of moderate hypertension and the absence of severe multiorgan damage.Lactate dehydrogenase (LDH) concentration in the severe form reached 656.1 ± 57.8 U /L, which is almost three times higher than the control values (225.0 ± 26.4 U /L, p < 0.001) and indicates severe tissue hypoxia and damage to cell membranes. In the moderate group, the LDH level was 545.9 ± 38.3 U /L, remaining significantly above the norm, indicating a persistent subclinical level of cytolysis.Overall, the obtained results demonstrate that severe preeclampsia is characterized by a combination of hypoproteinemia, hyperenzymemia, increasing azotemia, and a pronounced inflammatory response. Correlation analysis revealed a direct relationship between CRP levels and LDH values (r = 0.72, p < 0.01), as well as an inverse relationship between total protein concentration and the severity of cerebral changes according to MRI data (r = –0.58, p < 0.05), indicating a pathogenetic relationship between systemic inflammation, hemostatic disorders, and central nervous system damage in severe preeclampsia.
4. Conclusions
Summarizing all the data in our study, we can conclude that in pregnant women with severe preeclampsia, brain MRI reveals symmetrical hyperintense foci in the occipito-parietal regions, consistent with vasogenic edema. These changes are characteristic of posterior reversible encephalopathy syndrome (PRES), confirming the presence of systemic endothelial dysfunction and hypertensive CNS damage. Following stabilization of blood pressure and delivery, MR changes reverse, demonstrating the reversibility of cerebral dysfunction. Thus, the biochemical profile in pregnant women with preeclampsia of varying severity is characterized by increasing signs of multiple organ dysfunction as the disease worsens, consistent with clinical manifestations and MRI findings confirming the development of reversible encephalopathy.
References
| [1] | Stampalija T. et al. ISUOG Consensus Statement on maternal hemodynamic assessment in hypertensive disorders of pregnancy and fetal growth restriction // Ultrasound in Obstetrics & Gynecology. – 2025. – Т. 66. – №. 5. – С. 681. |
| [2] | Deng J. et al. Evaluating placental microstructure and microcirculation in predicting the progression of gestational hypertension to preeclampsia: a systematic comparison between virtual MR elastography, IVIM, ultrasound and lab indexes // Magnetic Resonance Imaging. – 2025. – Т. 122. – С. 110453. |
| [3] | Baadsgaard K. et al. T2* weighted fetal MRI and the correlation with placental dysfunction // Placenta. – 2023. – Т. 131. – С. 90-97. |
| [4] | Brzan Simenc G. et al. Correlation between cerebral biomarkers and optic nerve sheath diameter in patients with severe preeclampsia // Hypertension in Pregnancy. – 2021. – Т. 40. – №. 1. – С. 9-14. |
| [5] | Mahendra V., Clark S. L., Suresh M. S. Neuropathophysiology of preeclampsia and eclampsia: a review of cerebral hemodynamic principles in hypertensive disorders of pregnancy // Pregnancy Hypertension. – 2021. – Т. 23. – С. 104-111. |
| [6] | Qi Y. et al. The Association between pregnancy-induced hypertension and neonatal cerebral metabolism, hemodynamics, and brain injury as determined by physiological imaging // Frontiers in Physiology. – 2022. – Т. 13. – С. 756386. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML