-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(12): 4584-4586
doi:10.5923/j.ajmms.20251512.84
Received: Nov. 22, 2025; Accepted: Dec. 19, 2025; Published: Dec. 25, 2025

The Role of Cardiac Rhythm Variability and Autonomous Dysfunction in Predicting Aritmias in Oncological Patients Receiving Cardiotoxic Therapy
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLErgashov B. B.
Bukhara State Medical Institute, Bukhara, Uzbekistan
Correspondence to: Ergashov B. B., Bukhara State Medical Institute, Bukhara, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The study assessed the prognostic significance of heart rate variability and myocardial repolarization parameters in oncological patients receiving cardiotoxic chemotherapy. It has been established that a pronounced decrease in SDNN and RMSSD, an increase in the LF/HF ratio, and a prolongation of the QTc interval after 2-3 therapy cycles are reliably associated with the development of clinically significant and life-threatening arrhythmias. Patients with low heart rate variability were characterized by a significantly higher frequency of supraventricular and ventricular rhythm disturbances, as well as prolongation of QTc. The obtained data confirm the feasibility of including VSR analysis and QT-parameters dynamics in the cardiological monitoring protocol for early stratification of arrhythmogenic risk and improvement of antitumor treatment safety.
Keywords: Heart rate variability, Autonomic dysfunction, Heart arrhythmias, QT interval, QT dispersion, Chemotherapy, Cardiotoxicity, Oncological patients, Prognosis, Prevention
Cite this paper: Ergashov B. B., The Role of Cardiac Rhythm Variability and Autonomous Dysfunction in Predicting Aritmias in Oncological Patients Receiving Cardiotoxic Therapy, American Journal of Medicine and Medical Sciences, Vol. 15 No. 12, 2025, pp. 4584-4586. doi: 10.5923/j.ajmms.20251512.84.
1. Introduction
- Cardio-oncology as an interdisciplinary field has gained particular relevance against the backdrop of increasing cancer patient survival rates and expanding the use of potentially cardiotoxic anti-tumor regimens (anthracyclines, anti-HER2-therapy, tyrosine kinase inhibitors, immune checkpoint inhibitors). Heart rhythm disorders are often considered a frequent and prognostically unfavorable complication that can lead to the modification or discontinuation of antitumor treatment and worsen the outcome [1,2]. The ESC recommendations on cardio-oncology emphasize the need for active monitoring of cardiovascular complications during anti-tumor therapy, including arrhythmias and conduction disorders, using ECG monitoring and individual risk stratification [3].One of the promising non-invasive tools for early assessment of arrhythmogenic risk is the analysis of heart rate variability (HRV), which reflects the state of vegetative regulation and the balance of sympathetic/parasympathetic effects on the heart. HRV decrease is considered a marker of autonomous dysfunction and unfavorable cardiovascular prognosis, and in oncological patients, it can be formed both due to the tumor process itself and under the influence of antitumor treatment, inflammatory reactions, anemia, electrolyte imbalances, and drug interactions [4,5]. It has been shown that during chemotherapy, early changes in HRV can be detected according to daily Holter monitoring data, reflecting a decrease in the adaptive capabilities of the cardiovascular system even before the development of pronounced clinical manifestations [6].Autonomic dysfunction is particularly important during anthracycline therapy, for which changes in HRV indicators have been described, indicating disruption of autonomic regulation even in the early stages of treatment and in patients without a clear decrease in ejection fraction [7,8]. In immuno-oncological therapy, there is also high interest in the problem of arrhythmogenicity: immune-mediated cardiac complications, including myocarditis, are often accompanied by rhythm and conduction disorders, which requires increased vigilance and improvement of early risk detection methods [9].The aim of the study is to assess the role of heart rate variability and autonomic dysfunction indicators in predicting the development of arrhythmias in oncological patients receiving cardiotoxic anti-tumor therapy, with the aim of early stratification of arrhythmogenic risk and substantiation of preventive and monitoring approaches.
2. Materials and Methods of Research
- The study included patients ≥18 years old with confirmed oncopathology receiving cardiotoxic chemotherapy. Patients were divided into three groups: 1st group - standard management without preventive electrolyte correction; 2nd group - active monitoring and correction of K+ and Mg2+ levels before each cycle; 3rd group - combined prevention, including electrolyte correction and cardioprotective therapy (β-blockers, ACEI/ARB). All patients underwent a clinical examination, standard ECG registration with an assessment of the QT/QTc interval, and, if necessary, Holter ECG monitoring, echocardiography, as well as laboratory blood electrolyte levels.The main endpoints of the study were the frequency of electrolyte imbalance disorders, the frequency of heart arrhythmias, and the dynamics of the QTc interval. Statistical processing of the data was carried out using standard methods of variation statistics; the differences were considered statistically significant at p<0.05.
3. Research Results
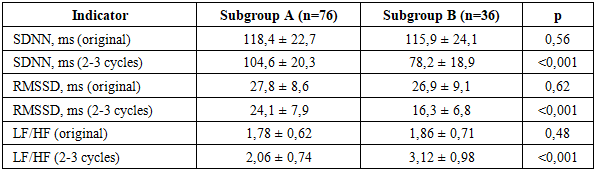
- The study assessed changes in autonomic regulation parameters (heart rate variability indicators, HRV) and myocardial repolarization (QTc, QT variance) in patients receiving cardiotoxic chemotherapy. To analyze the prognostic significance of the indicators, patients were divided into subgroups: subgroup A - without clinically significant arrhythmias (n=76) and subgroup B - with clinically significant or life-threatening arrhythmias (n=36). Additionally, an assessment of the influence of preventive approaches (1-3 groups) on the frequency of arrhythmias was conducted.Before starting therapy, no statistically significant differences were found between subgroups in SDNN, RMSSD, and LF/HF. After 2-3 cycles of chemotherapy, patients in subgroup B recorded a more pronounced decrease in SDNN and RMSSD, as well as an increase in LF/HF, reflecting increased sympathicotonia (Table 1).
|
|
|
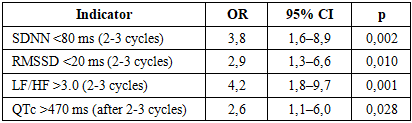
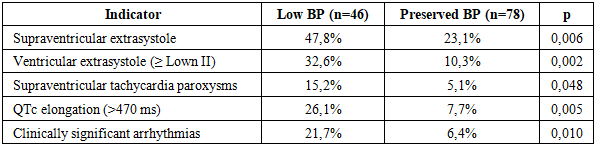
4. Conclusions
- The conducted research showed that in oncological patients receiving cardiotoxic chemotherapy, the development of arrhythmias is closely related to disorders in vegetative regulation and changes in myocardial repolarization processes. A pronounced decrease in heart rate variability indicators (SDNN and RMSSD) in combination with an increase in the LF/HF ratio and an increase in the QTc interval after 2-3 therapy cycles is a reliable predictor of clinically significant and life-threatening arrhythmias. Patients with low VSR are characterized by a significantly higher frequency of both supraventricular and ventricular rhythm disturbances, including prolongation of QTc. The obtained results substantiate the need for dynamic monitoring of HRV and QT/QTc parameters, as well as the implementation of preventive measures for early stratification of arrhythmogenic risk and improvement of the safety of antitumor treatment.