-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(12): 4581-4583
doi:10.5923/j.ajmms.20251512.83
Received: Nov. 27, 2025; Accepted: Dec. 21, 2025; Published: Dec. 25, 2025

Method for Determining Liver Biomarkers as Predicts of Chronic Heart Failure
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMakhmudova L. I., Rajabova Z. R.
Bukhara State Medical Institute, Bukhara, Uzbekistan
Correspondence to: Makhmudova L. I., Bukhara State Medical Institute, Bukhara, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The conducted study showed that chronic heart failure is accompanied by systemic organ disorders, the severity of which directly depends on the ejection fraction of the left ventricle. In patients with reduced blood pressure, higher levels of NT-proBNP, signs of cardiorenal dysfunction, and a significant increase in serum markers of liver fibrosis - collagen III and IV types - were detected. The obtained data indicate a significant role of chronic venous congestion and hypoxic damage in the formation of hepatic fibrosis in CHF. The use of extracellular matrix biomarkers in combination with clinical and instrumental indicators expands the possibilities of early diagnosis and prognostic assessment of organ complications, which can contribute to optimizing the management tactics of patients with various heart failure phenotypes.
Keywords: Сhronic heart failure, Ejection fraction, Type III collagen, Type IV collagen, Liver fibrosis, Venous congestion, Biomarkers
Cite this paper: Makhmudova L. I., Rajabova Z. R., Method for Determining Liver Biomarkers as Predicts of Chronic Heart Failure, American Journal of Medicine and Medical Sciences, Vol. 15 No. 12, 2025, pp. 4581-4583. doi: 10.5923/j.ajmms.20251512.83.
1. Introduction
- Chronic heart failure (CHF) with reduced left ventricular ejection fraction (LV EF <40%) is a severe clinical and pathophysiological form of cardiovascular pathology characterized by progressive heart pump failure, myocardial remodeling, and pronounced systemic effects on target organs [1,2]. According to the World Health Organization, the prevalence of CHF in developed countries is 2-4% of the adult population, while in the age group over 70 years - more than 10% [3]. In Uzbekistan, according to the statistics of the Ministry of Health (2023), the level of hospitalization due to decompensation of CHF is increasing annually, reflecting the growth in the number of patients with severe forms of the disease.One of the most vulnerable organs in CHF is the liver, whose function is impaired as a result of chronic congestion in the inferior vena cava system, decreased perfusion, and tissue hypoxia. This leads to the development of what is called "cardiogenic hepatopathy," or "heart liver," manifesting as cytolytic, cholestatic, and hypocoagulation syndromes [4,5].Laboratory indicators - biochemical markers of liver function (ALT, AST, IF, GGTP, bilirubin, albumin, INR) - are of particular importance, which, in combination with clinical symptoms, allow not only to assess the degree of liver damage but also to predict the severity and outcome of CHF [6,7]. Their change is associated with an increased risk of hospitalization, a deterioration in the quality of life, and an increase in mortality [8].Despite a large number of studies in the field of CHF, in the practice of primary care physicians, therapists, and cardiologists in Uzbekistan, the importance of laboratory assessment of liver function in cardiological practice is still underestimated. The lack of clear diagnostic and prognostic stratification algorithms using liver biomarkers leads to underestimation of the severity of the condition and insufficient optimization of therapy [9].The aim of the study is to determine the clinical and prognostic significance of biochemical markers of liver damage in patients with chronic heart failure with reduced left ventricular ejection fraction, with the aim of improving risk stratification, optimizing treatment tactics, and disease prognosis.
2. Materials and Methods of Research
- Clinical and laboratory studies were conducted at the Bukhara Multidisciplinary Medical Center between 2023 and 2024. The study included 98 patients who were hospitalized with a diagnosis of chronic heart failure (CHF), as well as 30 practically healthy individuals who constituted the control group.All patients were divided into two groups depending on the left ventricular ejection fraction (LVEF) determined by echocardiography data (using Simpson's method): • Group I (n = 55): patients with CHF and reduced LV ejection fraction (LV < 40%); • Group II (n = 43): patients with CHF and preserved LV ejection fraction (LV ≥ 50%). Clinical, laboratory, and instrumental examination of patients with CHF was conducted, assessing NYHA, EchoCG, ECG, and ultrasound, determining biochemical parameters, NT-proBNP, and serum markers of liver fibrosis (PIIINP, collagen IV, ELISA). Statistical analysis was performed in IBM SPSS 25.0 using correlation and ROC analysis at p<0.05.
3. Research Results
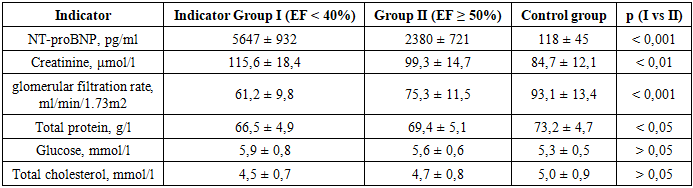
- Table 1 presents comparative laboratory and biochemical indicators in patients with chronic heart failure, depending on the left ventricular ejection fraction, as well as in the control group. The analysis was conducted to assess the severity of cardiorenal and metabolic imbalances with reduced and preserved myocardial systolic function (table 1).
|
|

4. Conclusions
- In patients with chronic heart failure, a decrease in left ventricular ejection fraction is associated with a significant increase in serum collagen levels of types III and IV, reflecting the progression of liver fibrous changes against a background of chronic venous congestion and hypoxia. Determining these markers allows for an objective assessment of the degree of liver damage and can be used for early stratification of the risk of hepatic complications in CHF.