-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(12): 4572-4574
doi:10.5923/j.ajmms.20251512.80
Received: Nov. 19, 2025; Accepted: Dec. 22, 2025; Published: Dec. 25, 2025

The Role of Electrolyte Balance Disorders in the Formation of Aritmias in Patients Receiving Chemotherapy: Clinical-Diagnostic Assessment and Preventive Approaches
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLErgashov B. B.
Bukhara State Medical Institute, Bukhara, Uzbekistan
Correspondence to: Ergashov B. B., Bukhara State Medical Institute, Bukhara, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

During the study, the role of electrolyte imbalance in the development of arrhythmias in patients with oncological diseases receiving cardiotoxic chemotherapy was assessed. It has been established that hypokalemia and hypomagnesemia significantly increase the risk of supraventricular and ventricular rhythm disturbances, as well as prolongation of the QTc interval. Active electrolyte correction significantly reduced the frequency of arrhythmias, while combined prevention, including electrolyte correction and cardioprotective therapy, completely prevented the development of clinically significant arrhythmias. The obtained results confirm the necessity of mandatory monitoring and preventive management of electrolyte disorders to improve the safety of chemotherapy in cancer patients.
Keywords: Heart arrhythmias, Chemotherapy, Cancer patients, Electrolyte balance, Hypokalemia, Hypomagnesemia, Cardiotoxicity, Prevention, Cardioprotection
Cite this paper: Ergashov B. B., The Role of Electrolyte Balance Disorders in the Formation of Aritmias in Patients Receiving Chemotherapy: Clinical-Diagnostic Assessment and Preventive Approaches, American Journal of Medicine and Medical Sciences, Vol. 15 No. 12, 2025, pp. 4572-4574. doi: 10.5923/j.ajmms.20251512.80.
1. Introduction
- The development of cardiotoxic complications in patients with oncological diseases against the background of antitumor therapy remains one of the most significant problems of modern cardiology. In the structure of these complications, heart rhythm disturbances occupy a special place, the frequency of which significantly increases when using anthracyclines, platinum-containing compounds, tyrosine kinase inhibitors, and immuno-oncological drugs [1,2]. According to major studies, therapy-induced arrhythmias are associated with increased mortality, decreased chemotherapy tolerance, and longer hospital stays [3,4].The main pathogenetic link in the formation of arrhythmias in this category of patients is the disruption of electrolyte balance, primarily the concentration of potassium, magnesium, and calcium. It is known that cisplatin and other platinum preparations cause pronounced hypomagnesemia and hypokalemia due to tubulopathy, and the frequency of hypomagnesemia can reach 70-90% with long courses of therapy [5,6]. Magnesium deficiency intensifies potassium loss, contributes to the prolongation of the QT interval, and significantly increases the risk of ventricular tachyarrhythmias, including torsade de pointes [7,8].The current recommendations of the European Society of Cardiologists emphasize the necessity of mandatory evaluation and timely correction of electrolytes in patients receiving cardiotoxic chemotherapy, especially when using drugs with the potential to prolong the QT interval [9]. It has been shown that maintaining potassium levels of >4.0 mmol/l and magnesium levels of >2.0 mg/dl significantly reduces the likelihood of developing serious arrhythmias and allows for safe continuation of antitumor treatment [10].The purpose of the study is to comprehensively assess the role of electrolyte imbalance in the formation of arrhythmias in patients receiving chemotherapy, to determine clinical and diagnostic predictors, and to develop well-founded preventive approaches to reduce the risk of therapeutic-induced heart rhythm disturbances.
2. Materials and Methods of Research
- The study included patients ≥18 years old with confirmed oncopathology receiving cardiotoxic chemotherapy. Patients were divided into three groups: 1st group - standard management without preventive electrolyte correction; 2nd group - active monitoring and correction of K+ and Mg2+ levels before each cycle; 3rd group - combined prevention, including electrolyte correction and cardioprotective therapy (β-blockers, ACEI/ARB). All patients underwent clinical examination, ECG with QT/QTc monitoring, and, if necessary, Holter monitoring, echocardiography, and laboratory analysis of electrolyte levels. The main outcomes were the frequency of arrhythmias and the dynamics of electrolyte balance; statistical data processing was carried out using standard methods, with a significance level of p<0.05.
3. Research Results
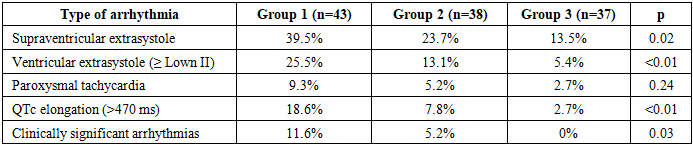
- The study included 118 patients, distributed as follows: Group 1 (standard management) - 43 patients; Group 2 (active electrolyte correction) - 38 patients; Group 3 (combined prevention) - 37 patients.The groups were comparable by age, sex, tumor localization, and chemotherapy types. The highest number of deviations was noted in the standard management group (Table 1).
|

|
4. Conclusions
- The conducted study showed that electrolyte imbalance is a significant and modifiable risk factor for developing arrhythmias in patients receiving cardiotoxic chemotherapy. The highest frequency of hypokalemia, hypomagnesemia, and associated arrhythmias was detected in the standard management group. Active electrolyte correction significantly reduced the frequency of both electrolyte disorders and arrhythmias, including prolongation of QTc. The greatest prophylactic effect was noted in a combined approach, including electrolyte correction and cardioprotective therapy: in this group, clinically significant arrhythmias and severe electrolyte disorders were practically absent. Thus, the implementation of comprehensive prevention significantly reduces the risk of therapy-induced rhythm disturbances and increases the safety of chemotherapy in cancer patients.