-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(12): 4569-4571
doi:10.5923/j.ajmms.20251512.79
Received: Dec. 3, 2025; Accepted: Dec. 22, 2025; Published: Dec. 25, 2025

Improvement of Non-Specific Ulcerative Colit Treatment Based on a Comprehensive Assessment of the Micronutrient Status
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMakhmudova L. I., Eshniyazova G. Sh.
Bukhara State Medical Institute, Bukhara, Uzbekistan
Correspondence to: Makhmudova L. I., Bukhara State Medical Institute, Bukhara, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

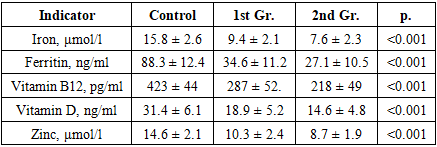
The study included 90 patients with NSUC and 30 healthy individuals; a comprehensive clinical-laboratory, endoscopic, and nutritional assessment was conducted, and targeted correction of deficiencies was carried out in some patients. Pronounced disorders in the levels of iron, ferritin, vitamins D and B12, and zinc were identified, statistically significantly correlating with the clinical and endoscopic activity of the disease. Conducting micronutrient correction contributed to a decrease in inflammatory markers, an improvement in the quality of life, a decrease in the activity of NSUC according to the Mayo scale, and an increase in the clinical effectiveness of therapy. The obtained results confirm the need to include a comprehensive assessment of micronutrient status in the standard algorithms for managing NSUC and demonstrate the high medical and practical significance of the developed method.
Keywords: Nonspecific ulcerative colitis, Micronutrient deficiency, Nutritional status, Vitamin D, Ferritin, Zinc, Calprotectin, Endoscopic activity, Individualized therapy
Cite this paper: Makhmudova L. I., Eshniyazova G. Sh., Improvement of Non-Specific Ulcerative Colit Treatment Based on a Comprehensive Assessment of the Micronutrient Status, American Journal of Medicine and Medical Sciences, Vol. 15 No. 12, 2025, pp. 4569-4571. doi: 10.5923/j.ajmms.20251512.79.
1. Introduction
- Non-specific ulcerative colitis (NSUC) is a chronic inflammatory disease of the colon with predominant mucosal involvement, prone to recurrent course, resistance to therapy, and the development of systemic complications. According to global statistics, the incidence of NSUC ranges from 9 to 20 cases per 100,000 population annually, with a steady growth trend both in developed countries and in transition economies, including Uzbekistan [1].NSUC primarily affects young and middle-aged individuals (20-40 years old), making it not only a medical but also a socio-economic problem. The prolonged course of the disease, frequent relapses, the need for expensive therapy and surgical interventions (15-20% of patients) create a high burden on the healthcare system and reduce the quality of life of patients [2].One of the underestimated, but extremely significant aspects in the pathogenesis and clinical course of NSUC is micronutrient deficiency. In patients with NSUC, nutritional status disorders are detected in 60-80% of cases, including iron, zinc, magnesium, vitamin D, B12, and folic acid deficiencies [3]. These disorders are caused by impaired absorption in the intestines, chronic blood loss, inflammation, and side effects of the drugs used (sulfasalazine, glucocorticoids, etc.). Micronutrient deficiency worsens the course of the disease, reduces the effectiveness of basic therapy, disrupts mucosal healing processes, and contributes to the formation of secondary complications (anemia, osteopenia, neuropathy) [4].Despite the high level of evidence in favor of identifying and correcting micronutrient deficiency in NSUC, in the practical healthcare of the Republic of Uzbekistan, this aspect remains outside the framework of standard clinical routes, and the nutritional status of patients is not systematically assessed. Thus, the lack of clear clinical and laboratory algorithms for diagnosing and correcting deficiency states in patients with NSUC limits the possibilities of personalized and pathogenetically justified therapy.The purpose of the study is to substantiate and develop a method for improving NSUC therapy based on a comprehensive assessment of micronutrient status and personalized correction of identified deficiencies.
2. Materials and Methods
- 90 patients with NSUC were examined, divided into two clinical groups (unoperated - 45 people; postoperative - 45 people) and 30 practically healthy volunteers. Assessment included clinical scales (Truelove-Witts, Mayo), general and biochemical blood analysis, micronutrient testing, calprotectin determination, endoscopic and histological methods. 30 patients underwent micronutrient correction.
3. Research Results
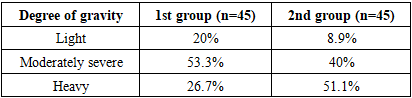
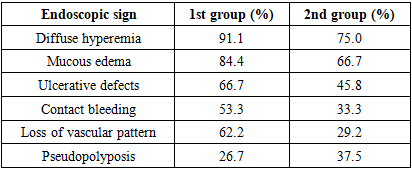
- The study included 90 patients with a confirmed diagnosis of NSUC and 30 practically healthy individuals who constituted the control group. Patients with NCA were divided into two clinical groups: unoperated patients (n=45) and patients who were in the postoperative period after colon resection or colectomy (n=45). The average age of the examined was 38.2±10.5 years; the proportion of men and women was 60% and 40%, respectively. The active phase of the disease was observed in 86.6% of patients, confirming the high frequency of recurrent and progressive NSUC course.When assessing the severity of the disease according to the Truelove-Witts scale, it was established that the moderate form of the disease prevailed in patients who did not undergo surgery, while in the second group (after surgery), severe forms of NSUC were observed significantly more often (Table 1).
|
|
|
|
|
4. Conclusions
- In patients with NSUC, a pronounced micronutrient deficiency develops, which significantly affects the severity of the disease and reduces the effectiveness of the ongoing therapy. Conducting a comprehensive assessment of nutritional status allows for the timely detection of such disorders that are not defined within the framework of standard diagnostic schemes. Inclusion of targeted correction of deficiency conditions in the treatment process leads to improvement of clinical symptoms, reduction of inflammation activity, and improvement of patients' quality of life. The developed method has proven high medical, social, and economic effectiveness and can be recommended for widespread implementation in practical healthcare.