-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(12): 4536-4539
doi:10.5923/j.ajmms.20251512.73
Received: Nov. 22, 2025; Accepted: Dec. 16, 2025; Published: Dec. 25, 2025

Comparative Analysis of the Dynamics of Quality of Life in Patients with Vestibulopathies
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMadmarov D. A.1, Usmanova D. D.2
1Central Asian Medical University, Fergana, Uzbekistan
2Tashkent State Medical University, Tashkent, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

A comparative analysis of the dynamics of the quality of life in 103 patients with central and peripheral vestibulopathies divided into groups in the conditions of inpatient treatment was carried out. Among the studied patient’s dizziness was accompanied by focal neurological symptomatology of different severity in the group of patients with central vestibulopathies. Moderately pronounced decrease in EF was observed with equal frequency in both groups. Intergroup comparison stated a highly significant correlation between diagnoses and clinical symptomatology of vertigo (χ2 = 34.65; p<0.001).
Keywords: Vestibulopathies, Central, Peripheral, Comparison, Quality of life
Cite this paper: Madmarov D. A., Usmanova D. D., Comparative Analysis of the Dynamics of Quality of Life in Patients with Vestibulopathies, American Journal of Medicine and Medical Sciences, Vol. 15 No. 12, 2025, pp. 4536-4539. doi: 10.5923/j.ajmms.20251512.73.
1. Introduction
- Among the numerous problems in neurology, disorders of the vestibular analyzer occupy a leading position, with particular emphasis placed on the detection of vestibular dysfunction.Vertigo is defined as “a sensation of disturbed orientation of the body in space or an illusory movement of one’s own body or the surrounding environment” [3,4].Vertigo is classified as being of central origin (involving lesions of the vestibular nuclei of the brainstem and their connections with other regions of the brain) or peripheral origin (resulting from damage to the vestibular nerve and the labyrinth) [5,6].In 2009, the International Bárány Society for Neuro-Otology presented standardized definitions of the main terms: vertigo (systemic, rotational dizziness), defined as a sensation of illusory movement of one’s own body or surrounding objects in space; dizziness (non-systemic, non-rotational dizziness), defined as a sensation of impaired spatial orientation without a false or distorted perception of movement; and imbalance or unsteadiness, defined as a sensation of postural instability of one’s own body while sitting, standing, or walking, without deviation of the body to a specific direction [9].It has been shown that approximately 2% of the adult population worldwide are admitted annually to emergency departments with moderate or severe symptoms of dizziness, with vestibular vertigo accounting for about one third of cases [10]. The prevalence of vestibular vertigo increases with age and occurs 2–3 times more frequently in women than in men [11].At the end of the last century (1998), J. R. Hotson and R. W. Baloh first introduced the term acute vestibular syndrome (AVS), which they defined as the sudden onset of continuous vertigo lasting more than 24 hours, accompanied by nausea and vomiting and exacerbated by head movements [8].However, even a quarter of a century later, many aspects of the differential diagnosis of the etiology of acute vertigo remain highly complex and unresolved [13].Isolated vertigo is often caused by pathology of the central components of the vestibular analyzer associated with small focal ischemic lesions in the region of the inferior cerebellar peduncle, the nodulus, or at the level of the entry zone of the VII cranial nerve into the brainstem, that is, at the junction of the pons and the medulla oblongata [12].In recent years, a global trend toward an increasing number of patients with vestibulopathies has been observed. Most studies by international authors focus on assessing vestibular function in elderly individuals, whereas investigations involving younger patients remain insufficient. This is often attributed to limitations in diagnostic technologies and a lack of qualified vestibular specialists in outpatient and inpatient healthcare settings.Aim of the study: to comparatively assess the dynamics of quality of life in patients with central and peripheral vestibulopathies.
2. Materials and Methods
- During the period from 2023 to 2024, 103 patients (59 men and 44 women) with central and peripheral vestibulopathies aged 30–59 years were examined, corresponding to young and middle age according to the WHO classification [2]. The mean age of the study population was 49.25 ± 8.03 years. The mean age of men was 49.20 ± 8.44 years (range: 31–59 years), while the mean age of women was 49.29 ± 7.78 years (range: 30-59 years).The patients’ medical and life histories, complaints, and somatic status were evaluated. To differentiate between peripheral and central origins of vertigo, positional tests were performed, including the Romberg test, finger-to-nose test, and assessment of straight-line and tandem gait. In addition, the Dix–Hallpike test, McClure-Pagnini test, Halmagyi-Curthoys head impulse test (HIT), Unterberger (Fukuda) stepping test, and the alternate cover test were conducted.To objectively assess the intensity of vertigo and imbalance and their impact on quality of life before and after treatment for autonomic insufficiency, the visual analog scale for vertigo (VAS-V) and the Dizziness Handicap Inventory (DHI) were used [7]. The obtained results were subjected to appropriate statistical analysis using standard methods.
3. Results and Discussion
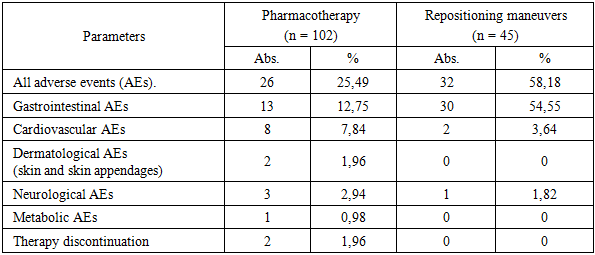
- The time of symptom onset was determined for all 103 patients. Of these, 83 patients (80.58% of the total) 47 patients (83.93%) in Group I and 36 patients (76.60%) in Group II were admitted within the first 12 hours of symptom onset. Between 12 and 24 hours after symptom onset, 20 patients (19.42% of the total) 9 patients (16.07%) in Group I and 11 patients (23.40%) in Group II were hospitalized.The main complaints among patients in both groups were vertigo reported by 94 patients (91.26%) and nausea reported by 70 patients (67.96%) against a background of spatial imbalance, noted in 73 patients (70.87%), and headache, reported by 91 patients (88.35%). Additional symptoms included weakness in 80 patients (77.67%), disorientation in 56 patients (54.37%), and visual disturbances such as blurred vision, darkening of the eyes, and flickering of objects with indistinct contours in 42 patients (40.78%).In Group I, vertigo was reported by 51 patients (91.07%), nausea by 41 patients (73.21%), spatial imbalance by 43 patients (76.79%), headache by 56 patients (100%), weakness by 42 patients (75.00%), disorientation by 30 patients (53.57%), and visual disturbances by 22 patients (39.29%) of the group members.In Group II, vertigo was reported by 43 patients (91.49%), nausea by 29 patients (61.70%), spatial imbalance by 30 patients (63.83%), headache by 35 patients (74.47%), weakness by 38 patients (80.85%), disorientation by 26 patients (55.32%), and visual disturbances by 20 patients (29.79%) of the group members.It should be noted that there was a statistically significant difference in complaints of tinnitus (1 patient [1.79%] in Group I versus 35 patients [74.47%] in Group II) (P < 0.0001) and headache (56 patients [100%] in Group I versus 35 patients [74.47%] in Group II) (P < 0.05). Thus, these two symptoms have differential diagnostic significance.Correlation analysis revealed an association between the age and sex of patients with vestibulopathies and the frequency of clinical manifestations (−0.42 < r < 0.59).We analyzed the established clinical diagnoses in the vestibulopathy groups. In Group I, the predominant diagnosis was ischemic stroke in the vertebrobasilar basin (VBB) in 48 patients (85.71%), of which 27 patients (56.25%) had a first-ever event and 21 patients (43.75%) had a recurrent cerebrovascular accident. The remaining 8 patients (14.29%) were diagnosed with a transient ischemic attack (TIA) in the VBB. In Group II, two clinical diagnoses were identified: acute positional vestibulopathy (APV) in 35 patients (74.47%) and benign paroxysmal positional vertigo (BPPV) in 12 patients (25.53%).In the subjective assessment of vertigo using the VAS-V scale, the mean score in Group I was 7.41 ± 0.72 points, while in Group II it was 8.93 ± 0.74 points, showing no statistically significant difference (p = 0.144141).According to the DHI scale, the mean group scores at admission were 46.74 ± 9.17 points in Group I and 54.82 ± 9.36 points in Group II, which also did not reach statistical significance (p = 0.067). However, it is noteworthy that there were no patients with severe vertigo in Group I, whereas 11 patients (23.40%) in Group II presented with severe vertigo (χ² with Yates correction = 12.098, P < 0.001; Fisher’s exact test = 0.00010, P < 0.05).The Pearson coefficient (C') was 0.498, indicating a relatively strong correlation between the severity of vertigo according to DHI and the etiology of vertigo.A moderately reduced quality of life was observed with equal frequency in both groups. It should be noted that severe impairments were more prevalent in Group II, which we attributed to the patients’ emotional responses.Based on her work, L. M. Antonenko concluded that “patients with vestibular disorders may range from calmly observing their symptoms to experiencing anxiety of varying intensity and forms, which significantly aggravates the course of the disease—often presenting as pronounced anxiety-depressive disorders or developing into phobic postural instability” [1].In the comprehensive treatment of vestibulopathies, pharmacotherapy, repositioning maneuvers, and vestibular rehabilitation are commonly used, while surgical correction and artificial support devices are less frequently applied.The majority of patients in our study—102 individuals (99.03%)—received pharmacotherapy, with 55 patients (53.4%) receiving it as part of a combination treatment. The most widely used pharmacological group was histamine mimetics, specifically betahistine dihydrochloride, administered to 54 patients (52.43%).Repositioning maneuvers and vestibular rehabilitation (VR) were applied in 55 patients (53.40%), with 47 patients (45.63%) receiving VR alone. In Group II, VR was prescribed to 45 patients (95.74%), and repositioning maneuvers were performed in 12 patients (25.53%) with BPPV.Additionally, in Group II, H1-antihistamines (dimenhydrinate) were administered to 41 patients (87.23%), antiemetics (metoclopramide) to 35 patients (74.47%), and histamine mimetics (betahistine dihydrochloride) to 27 patients (57.45%).It should be noted that the most effective method for managing acute vestibular syndrome (AVS) was repositioning maneuvers in patients with BPPV, successfully applied in 12 patients (100%).Thus, the highest efficacy in controlling AVS within the first day of symptom onset was observed in the group of patients with peripheral vestibulopathies. The lowest effectiveness of the comprehensive therapy was demonstrated in 21 patients (43.75%) from Group I, who had recurrent ischemic strokes in the vertebrobasilar basin and central autonomic insufficiency.
|

|
4. Conclusions
- 1. In the differential diagnosis and management of patients with vestibulopathies, they should be classified according to the topographic-pathogenetic origin into central and peripheral vestibulopathies, with mandatory evaluation to diagnose or exclude life-threatening conditions such as acute cerebrovascular accidents (ACVA).2. In patients with central and peripheral vestibulopathies, the initial quality of life (QoL) assessed by VAS-V is significantly worse in cases of peripheral origin. After one day of therapy, QoL is lower in the group with central vestibulopathies, although the difference compared to peripheral vestibulopathies is not statistically significant. In both groups, there is a statistically significant improvement compared to baseline, with symptom regression being more pronounced in peripheral vestibulopathies.3. According to the DHI scale, mean group scores in central and peripheral vestibulopathies showed no statistically significant differences either at baseline or after one week of therapy, both in intergroup comparisons and when compared with baseline values within each group.4. The use of glucocorticoids in the treatment of acute vestibular syndrome and repositioning maneuvers with a low rate of adverse events is recommended, given the significant number of patients with acute positional vestibulopathy (APV) and benign paroxysmal positional vertigo (BPPV) in neurological departments.