Abdukhakim Muminovich Khadjibaev1, Erkin Yuldashevich Valiev2, Fayzulla Khamidullaevich Mirjalilov3, Zafar Raimovich Khasanov4, Begzod Rakhmadjanovich Karimov4, Alisher Takhirovich Tukhtapulatov5
1MD, Professor, Republican Scientific Center for Emergency Medical Care, Tashkent, Uzbekistan
2MD, Professor, Head of the Clinical Department of Traumatology, Republican Scientific Center for Emergency Medical Care, Tashkent, Uzbekistan
3Head of the Adult Traumatology Department, Republican Scientific Center for Emergency Medical Care, Tashkent, Uzbekistan
4Adult Traumatology Department, Republican Scientific Center for Emergency Medical Care, Tashkent, Uzbekistan
5Traumatologist, Tashkent Clinical Hospital for Emergency Medical Care, Tashkent, Uzbekistan
Correspondence to: Abdukhakim Muminovich Khadjibaev, MD, Professor, Republican Scientific Center for Emergency Medical Care, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
This article is devoted to improving the tactics of treatment of combined skeletal trauma complicated by fat embolism syndrome, which is one of the main causes of death in severe combined skeletal trauma. A single-centre study including 236 patients with combined trauma complicated by fat embolism was performed. 97 patients were in control group and received conventional therapy, 139 patients of main group undergone modern “damage control orthopedics” tactics. The authors developed and introduced into the practice of treating such patients original modern minimally invasive technologies, improved the treatment regimen for fat embolism. Modern interventions in main group significantly reduced the invasiveness and aggressiveness of interventions in patients with combined trauma and resulted in decrease of hospital stay and incidence of complications.
Keywords:
Combined skeletal trauma, Fat embolism, Damage control orthopedics
Cite this paper: Abdukhakim Muminovich Khadjibaev, Erkin Yuldashevich Valiev, Fayzulla Khamidullaevich Mirjalilov, Zafar Raimovich Khasanov, Begzod Rakhmadjanovich Karimov, Alisher Takhirovich Tukhtapulatov, Results of Treatment of Patients with Skeletal Trauma Complicated by Fat Embolism Syndrome, American Journal of Medicine and Medical Sciences, Vol. 15 No. 12, 2025, pp. 4446-4451. doi: 10.5923/j.ajmms.20251512.54.
1. Introduction
Due to intensive urbanization, industrial development, urban development, the expansion of the automobile fleet, natural and man-made disasters, and military action, the number of victims with severe combined skeletal trauma (SCT) has increased worldwide in the past decade [2,4,15,21].In recent years alone, the incidence of SCT has reached 17.5-28.0% of all patients in trauma hospitals. According to the World Health Organization (WHO), the mortality rate for SCT is 25-60%, ranking third in the overall mortality rate from noncommunicable diseases [5,8,10,17]. Fat embolism syndrome (FES), characterized by multiple occlusion of blood vessels by fat emboli (fat droplets, undifferentiated lipid masses, fat cells, or lipid complexes larger than 7–8 μm) with the development of multiple organ failure (MOF) [7,9,11,12,18,19,20], occupies a significant place among the main causes of mortality in severe skeletal trauma, along with acute blood loss, traumatic hemorrhagic shock, and complications of traumatic brain injury.These conditions include the development of multiple organ failure (MOF) [7,9,11,12,18,19,20].The above data provide objective justification for further in-depth research into the prevention and treatment of FES in associated skeletal injuries.
2. Purpose of the Research
The aim of this study is to improve the treatment outcomes for severe skeletal injuries associated with FES through the use of minimally invasive surgical correction techniques and improved prevention methods for these complications.
3. Materials and Methods
This study is based on an analysis of diagnostic and treatment results for 236 patients with severe skeletal injuries complicated by the development of FES, who were seen in the trauma and intensive care departments of the Russian Scientific Center for Emergency Medicine from 2008 to 2022.There were 192 men (81.4%) and 44 women (18.6%), with an average age of 43.8 ± 3.6 years. Depending on the treatment strategy and preventive procedures, all patients with FES were divided into two groups: a control group and a study group.The control group included 97 patients (41.1%) who received traditional treatment according to the principles of "early total care," i.e., maximum performance of all treatment procedures for injuries and standard preventive procedures. In contrast, 139 (58.9%) patients in the study group received treatment consistent with the current doctrine of damage control orthopedics (DCO) for the correction of combined skeletal injuries, with the widespread use of minimally invasive surgical interventions. Furthermore, in the study group, we used an optimized regimen for the prevention of FES by incorporating a succinic acid solution.During the study, general clinical, laboratory, and instrumental (X-ray, MSCT, MRI) examinations, as well as biomedical statistics, were used in accordance with diagnostic standards adopted at the Russian Scientific Center for Emergency Medicine.
4. Results
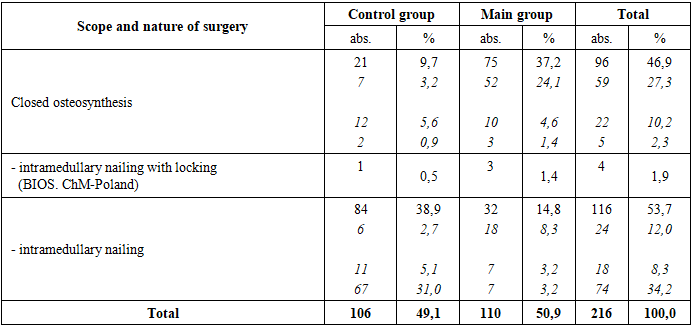
Patients in the control and study groups with combined skeletal trauma complicated by FES were transported to the emergency shock unit in accordance with the "golden hour" rule. They were examined by a surgeon, anesthesiologist-resuscitator, neurosurgeon, and traumatologist. During the first 15 minutes, measures were taken to ensure the preservation of vital functions (definitive cessation of external bleeding, elimination of asphyxia, restoration/maintenance of the upper airway (UA), oxygen therapy, tracheal intubation and artificial ventilation as indicated, cardiopulmonary resuscitation, catheterization of the main veins and bladder, initiation of infusion-transfusion anti-shock therapy, and pain relief).In parallel, the necessary diagnostic procedures were performed. Each specialist addressed their own professional needs; overall leadership and team coordination at the initial stage was provided by a general multidisciplinary surgeon, selected from among the most trained specialists.After Before diagnosis, patients underwent various surgical interventions. A total of 97 patients in the control group and 139 in the study group with combined skeletal injuries complicated by FES were analyzed.In these patients, we performed a total of 216 different traumatological interventions to correct existing combined skeletal and abdominal injuries.The scope and types of skeletal injury correction surgeries performed in both groups are presented in Table 1.Table 1. Volume and type of skeletal injury surgeries in the examined patients, n=216
 |
| |
|
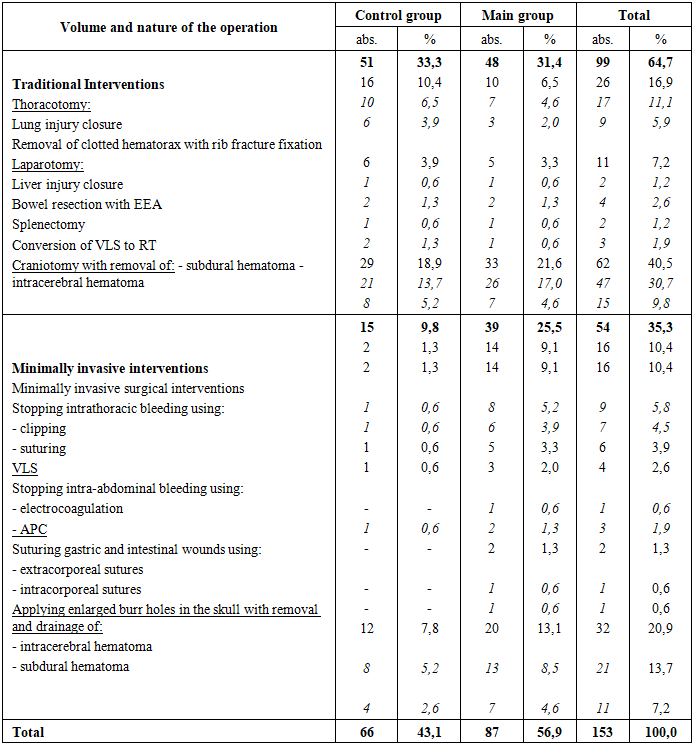
As can be seen from the data presented in Table 1, all patients underwent correction of existing bone fractures using closed (96) and open (116) osteosynthesis techniques. Osteosynthesis was performed using both conventional methods of intramedullary osteosynthesis with pins (40) and external osteosynthesis (74), as well as a modern method of intramedullary osteosynthesis with locking (BIOS. ChM-Poland) (83). In particularly complex cases of intra-articular fractures of the tibia and forearm (5), we used external hardware fixation. In 4 patients with pelvic fractures, closed stabilization of the injuries was performed using the clinic's apparatus.It should be noted that in patients in the control group, open osteosynthesis was considered the primary method of correction of skeletal injuries, which was used in the majority of such patients (38.9%). In contrast, in patients in the main group, we extensively used closed osteosynthesis (37.2%) to correct existing skeletal injuries using the modern BIOS pin, which allows for simultaneous pinning and fracture blocking.In addition to the above-mentioned trauma surgeries, we performed surgical correction of various combined cavitary injuries in 216 patients examined. The extent and type of cavitary injury surgeries performed in the examined patients are presented in Table 2.Table 2. Extent and type of cavitary injury surgeries performed in the examined patients, n=216
 |
| |
|
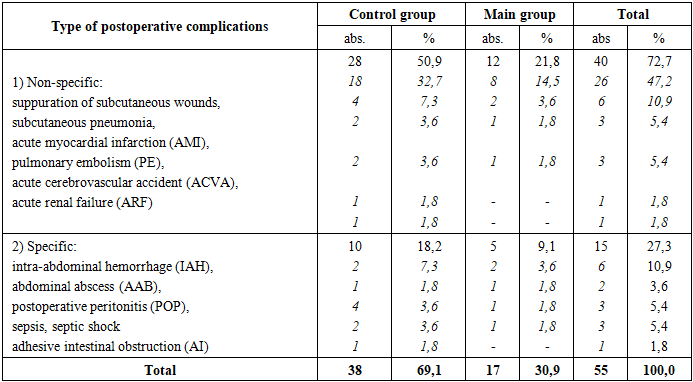
As can be seen from the data presented in Table 2, in 66 patients in the control group, stabilization of existing combined cavitary injuries, as well as skeletal injuries, was performed using traditional methods in 33.3% of cases. Moreover, in these patients, we used a treatment strategy based on the principles of "early total care" (ETC) as much as possible (up to 84.3%), meaning that surgical interventions were performed simultaneously and sequentially by multiple teams of surgeons and traumatologists.Thus, traditional thoracotomies (TT) combined with stabilization of existing limb fractures were performed in 16 patients, with 10 of these patients undergoing suturing of lung injuries, 6 patients undergoing removal of clotted hemothorax with fixation of existing rib fractures, and all of these patients completed the procedure with debridement and drainage of the pleural cavities.In 6 patients in the control group, stabilization of existing limb fractures was combined with traditional laparotomy. During the latter procedure, liver injuries were sutured in 1 patient. Two patients underwent bowel resection with an entero-enteroanastomosis. One patient underwent splenectomy; all abdominal surgeries were completed with debridement and drainage of the abdominal cavity.Forty-one patients in the control group had limb fractures associated with traumatic brain injury. These were corrected in 29 of these patients using traditional decompressive craniotomy. Subdural (21) and intracerebral (8) hematomas were removed.In 14.8% of patients in the control group, existing injuries required more than two surgical interventions. In cases of combined chest and abdominal injuries, we primarily performed correction of intrapleural injuries with decompression.All patients in the control group, along with surgical correction of various associated injuries, received traditional treatment for the existing complication of FES.The drug component of which included oxygen insufflation (non-invasive CPAP method or prolonged mechanical ventilation), infusion therapy for systemic microcirculation disorders, dehydration therapy (glycerol 10% - 0.5 g / kg), correction of cerebral hypoxia (GHB), nootropic and metabolic therapy (cerebrolysin, glutamic acid, actovegin), correction of the coagulation system (heparin 20-30 thousand units / day), hormonal therapy, high doses of protease inhibitors - contrical (300 thousand units / day), the use of lipotropic drugs and substances that prevent lipid demulsification (Essentiale, glucose-alcohol solutions), parenteral and enteral nutrition, antibacterial therapy. Unlike the control group, in patients in the study group, we used a staged treatment approach in accordance with the modern doctrine of damage control orthopedics (DCO) for the correction of combined skeletal injuries in 25.5% of patients, as in cases of skeletal fractures. We utilized modern minimally invasive technologies for surgical interventions to eliminate combined skeletal and cavitary injuries in patients in the study group.For example, in 14 patients in the study group, we corrected combined intrapleural organ injuries using videothoracoscopy. In all cases, the interventions included stopping intrathoracic bleeding by clipping (8) and suturing (6), followed by debridement and drainage of the pleural cavity.In five patients in the study group, we corrected combined intra-abdominal injuries using videothoracoscopy. Surgical interventions included stopping bleeding from liver injuries using electrocoagulation (1) and argon plasma coagulation (2). In two patients, videolaparoscopic suturing of stomach and intestinal injuries was successful, using extracorporeal (1) and intracorporeal (1) sutures.We corrected combined traumatic brain injury in 20 patients by removing subdural (13) or intracerebral (7) hematomas through enlarged burr holes.It should also be noted that the drug therapy regimen for patients in the main group was supplemented with the following mixture: succinic acid 2.0 g, sodium chloride 6.2 g, potassium chloride 0.3 g, calcium chloride 0.082 g, magnesium chloride 0.1 g, sodium bicarbonate 3.0 g, and water for injection up to 1 liter.In the postoperative period, various specific and non-specific complications were observed in the control and study groups of patients with combined skeletal injuries and FES.The types of postoperative complications in these patients are presented in Table 3.Table 3. Postoperative complications in the control and study groups of patients with combined skeletal injuries and FES, n=55
 |
| |
|
A total of 38 patients in the control group (69.1%) experienced various postoperative complications of a nonspecific and specific nature. Nonspecific complications were observed in only 28 patients. These included postoperative wound suppuration (18), postoperative pneumonia (4), acute myocardial infarction (2), pulmonary embolism (2), stroke (1), and acute renal failure (1). Nonspecific complications were managed conservatively in the vast majority of cases.Specific postoperative complications were observed in a total of 10 patients in the control group. Among the specific surgical complications, the most common were ongoing PP (2) and ALP (1) of various locations. Relatively fewer cases involved IBD (2) and SCI (1). A distinctive feature of specific postoperative complications was that their correction required repeat surgical interventions in almost all cases. The average hospital stay in the control group was 38.2 ± 2.7. A total of 12 (12.4%) patients in the control group died in the postoperative period. The causes of death included anastomotic suture failure and peritonitis (4), multiple organ failure secondary to sepsis with severe intoxication or bleeding (2), pulmonary embolism (1), FES (4), and acute myocardial infarction (1). It should be noted that patients in the control group had high rates of both severe FES (32) and mortality among this cohort of patients (12.5%).A total of 17 patients in the study group (30.9%) experienced various postoperative complications of a nonspecific and specific nature. In the postoperative period, patients in the study group experienced significantly fewer nonspecific and specific complications than those in the control group, despite virtually identical rates of nonspecific and specific complications. In this regard, a decrease in the incidence of severe FES (17) and mortality among this patient group (5.9%) is noteworthy in the study group.This was most likely due, firstly, to the expansion of indications for the use of MIT in these patients and a significant reduction in the morbidity of surgical interventions, and secondly, to improvements in the FES treatment regimen.The average hospital stay in the study group was 21.3 + 1.6. A total of 4 patients (2.8%) died in the postoperative period in the study group. The causes of death were anastomotic suture failure and peritonitis (2), FES (1), and pulmonary embolism (1). The rate of good and satisfactory treatment outcomes in the study group was 1.75 times higher than in the control group.
5. Discussion
Currently, the overall structure of peacetime trauma shows an increase in the incidence of combined injuries to 60-70%, accompanied by 49.8% to 83.5% of musculoskeletal injuries. Among musculoskeletal injuries, limb injuries predominate (52.2%-86.6%), with long bone fractures being the most typical, occurring in 56.2%-86% of cases [6,8,13].One of the serious complications of the aforementioned skeletal injuries is fat embolism syndrome, which causes fatal outcomes in 1% to 15% of cases [1,2,14,16].This study was devoted to a comparative analysis of traditional and improved treatment tactics for patients with combined skeletal injuries complicated by FES.A comparative analysis of treatment outcomes between the control and study groups of patients clearly demonstrated that, thanks to the use of improved treatment tactics in patients with combined skeletal injuries, the proportion of staged surgeries in accordance with the modern "damage control orthopedics" (DCO) doctrine has increased, along with expanded capabilities for the use of modern MIT in the form of VLS, VTS, intracranial interventions using enlarged burr holes, and minimally invasive trauma techniques.The latter, due to their simultaneous adequacy and minimally invasiveness, significantly reduce the trauma and aggressiveness of interventions in patients with combined skeletal injuries. This is reflected in a significant increase in the number of good (up to 37.4%) and satisfactory (up to 42.4%) treatment outcomes in the study group compared to the control group.
6. Conclusions
All of the above data are clearly reflected in a reduction in the number of postoperative complications, a decrease in mortality, and a reduction in the number of days spent in hospital.The implementation of the proposed improved tactics for the treatment of combined skeletal injuries complicated by SFE in the practical activities of the Department of Combined Injuries of the Russian Scientific Center for Emergency Medicine, its branches and subbranches will improve the effectiveness of treatment and reduce the incidence of postoperative complications.
References
| [1] | Dats A. V., Dats L. S., Khmelnitsky I. V. The structure of defects in the provision of medical care for polytrauma in intensive care units // Polytrauma. – 2017. – no. 3. – P. 23-29 (in Russian) |
| [2] | Dmitriev I. V., Dorosevich A. E. Fat embolism: history and terminological features // Ural medical journal. – 2017. – no. 4. - S. 88-92. (in Russian) |
| [3] | Kukharev D.I. Forensic diagnostics of complications in associated trauma / D.I. Kukharev, A.A. Sverchinskaya, E.A. Evenings [and others] // Young scientist. - 2018. - No. 16. - P. 36-38. (in Russian) |
| [4] | Likhterman L.B. Consequences of traumatic brain injury /L.B. Likhterman, A.A. Potapov, V.A. Klevno et al. // Forensic Medicine. The science. Practice. Education. - 2016. - V.2, No. 4. - P. 4 - 20. (in Russian) |
| [5] | Markosyan S.A. Comparative analysis of the causes and nature of car injuries in children who received outpatient care in 2014 and 2015 // Scientific almanac. – 2017. – no. 1-3. – S. 209-213. (in Russian) |
| [6] | Pankov I.O., Sirazitdinov S.D. Fat embolism syndrome as the main cause of mortality in severe polytrauma // Modern problems of science and education. – 2015. – no. 2. - S. 83-93. (in Russian) |
| [7] | Razzokov A. A., Nazarov M. K. Differential diagnosis of severe concomitant traumatic brain injury and fat embolism syndrome // Bulletin of Avicenna. - 2017. - T. 19. - No. 3. (in Russian) |
| [8] | Firsov C.A. Features of modern traumatism: pathogenetic, therapeutic and organizational aspects / S.A. Fipcov, R.P. Matveev, N.A. Vereshchagin [and others]. - Apxangelsk: Publishing House of the Northern State. honey. un-ta, 2016. - 297 p. (in Russian) |
| [9] | Yakovlev A.Yu. Fat embolism: textbook / A.Yu. Yakovlev, S.A. Tezyaeva, V.V. Kichin, V.O. Nikolsky, A.A. Pevnev. - Nizhny Novgorod: Institute of the FSB of Russia, 2016. - 112 p. (in Russian) |
| [10] | Butcher, N.E. The definition of polytrauma: the need for international consensus / N.E. Butcher, N. Enninghorst, K. Sisak [et al.] // J Trauma Acute Care Surg. – 2013. – Vol.74, №3.- P. 884-889. |
| [11] | Caricato, A., Russo, G., Biasucci, D. G., & Annetta, M. G. Fat embolism syndrome // Intensive care medicine. – 2017. – Т. 43. – №. 9. – С. 1411-1412. |
| [12] | Dahl, O. E., Reikerås, O., Pripp, A. H., & Engesæter, L. B. Fat embolism is an outdated diagnosis // Tidsskrift for den Norske laegeforening: tidsskrift for praktisk medicin, ny raekke. – 2018. – Т. 138. – №. 4. |
| [13] | David C. Changes in the epidemiology and prediction of multipleorgan failure after injury // C. David, M. Seth, L. Kate, J. Zsolt // Journal of Trauma and Acute Care Surgery. – 2013.– Vol. 74. – P. 774–779. |
| [14] | Graziani A., Moretti C. C., Cappa F. M. Fat embolism syndrome: chest CT findings //Jornal Brasileiro de Pneumologia. – 2018. – Т. 44. – №. 3. – С. 244-244. |
| [15] | Gross, T. Long-term outcome following multiple trauma in working age: A prospective study in a Swiss trauma center / T. Gross, F. Amsler // Unfallchirurg. – 2016. – Vol. 119, №3. - P. 921-928. |
| [16] | Guerado, E., Bertrand, M. L., Cano, J. R., Cerván, A. M., Galán, A. Damage control orthopaedics: State of the art // World journal of orthopedics. – 2019. – Т. 10. – №. 1. – С. 1. |
| [17] | Hierro-Cañas, F. J., Andrés-Cano, P., Rabadán-Márquez, G., Giráldez- Sánchez, M. A., & Cano-Luis, P. Fracturas de astrágalo. Resultados funcionales en pacientes politraumatizados // Revista Española de Cirugía Ortopédica y Traumatología – 2019. |
| [18] | Malgapo K. K. L., Osman C., Prevett M. Cerebral fat embolism: the value of susceptibility-weighted imaging. – 2018. |
| [19] | Renninger, C. H., Cochran, G., Tompane, T., Bellamy, J., & Kuhn, K. Injury characteristics of low-energy Lisfranc injuries compared with high-energy injuries // Foot & ankle international. – 2017. – Т. 38. – №. 9. – С. 964-969. |
| [20] | Rozema, R., Doff, M. H., van Ooijen, P. M., Postmus, D., Westerlaan, H. E., Boomsma, M. F., & van Minnen, B. Diagnostic reliability of low dose multidetector CT and cone beam CT in maxillofacial trauma—an experimental blinded and randomized study // Dentomaxillofacial Radiology. – 2018. – Т. 47. – №. 8. – С. 20170423. |
| [21] | Simmel S. Long-term results after multiple trauma with ISS ≥ 25. Outcome and predictors of quality of life / S. Simmel, S. Drisch, S. Haag [et al.] // Chirurg. – 2013. – Vol. 84, № 9. - P. 771-779. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML