Jalilov Gulomjon Mirvoxidovich1, Khodjiyev Bakhriddin Farkhodjonovich1, Mirzaxmedova Dilfuza Marufovna1, Jin-Tae Kim2, Yusupov Anvar Sobirovich2, Xaydarov Qambarali Imomaliyevich3
1Department of Anesthesiology and Pain Medicine, National Children’s Medical Center, Tashkent, Uzbekistan
2Department of Anesthesiology and Pain Medicine, Seoul National University Hospital, Jongno-gu, Seoul, Republic of Korea
3Department of Cardiac Surgery, Children's Clinic, Tashkent State Medical University, Tashkent, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Routine use of intraoperative transesophageal echocardiography (TEE) is a safe monitoring and diagnostic method during pediatric congenital cardiac surgery. However, the question of whether intraoperative TEE is accurate and cost effective for patients with tetralogy of Fallot (TOF) has not been raised. This study aimed to analyze the cost-benefit of routine TEE during the repair of TOF.
Keywords:
Tetralogy of fallot, Transesophageal echocardiography, Surgery
Cite this paper: Jalilov Gulomjon Mirvoxidovich, Khodjiyev Bakhriddin Farkhodjonovich, Mirzaxmedova Dilfuza Marufovna, Jin-Tae Kim, Yusupov Anvar Sobirovich, Xaydarov Qambarali Imomaliyevich, The Role of Intraoperative Transesophageal Echocardiography in Predicting Surgical Outcomes in Patients with Tetralogy of Fallot, American Journal of Medicine and Medical Sciences, Vol. 15 No. 12, 2025, pp. 4441-4445. doi: 10.5923/j.ajmms.20251512.53.
1. Introduction
Tetralogy of Fallot (TOF) represents the most prevalent cyanotic congenital heart defect in pediatric populations, characterized by a constellation of four anatomical anomalies: ventricular septal defect (VSD), overriding aorta, right ventricular outflow tract (RVOT) obstruction, and right ventricular hypertrophy. The surgical correction of TOF demands exceptional precision and real-time monitoring to ensure optimal outcomes. Intraoperative transesophageal echocardiography (TEE) has emerged as an indispensable diagnostic and monitoring tool in cardiac surgery, providing unparalleled real-time visualization of cardiac structures and function during surgical procedures [2,7,11].This comprehensive retrospective study was conducted at the National Children's Medical Center (Tashkent, Uzbekistan) between January 2022 and April 2025. The investigation aimed to evaluate the efficacy of TEE in 129 pediatric patients who underwent radical correction for TOF, with particular emphasis on postoperative outcomes, hemodynamic stability, and complication rates [5].
2. Objective and Methodology
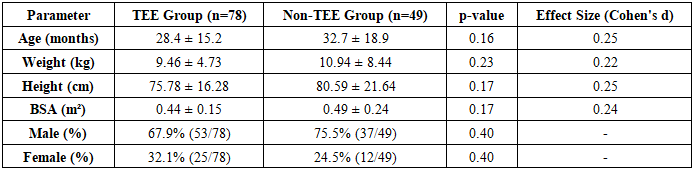
Primary Objective: To rigorously test the hypothesis that the utilization of intraoperative TEE significantly improves surgical outcomes of radical correction for TOF through advanced statistical methods and comparative analysis.Secondary Objectives: To assess the impact of TEE on postoperative hemodynamic stability.To evaluate the reduction in complication rates with TEE guidance. To analyze the economic implications of TEE utilization through reduced ICU stay and reoperation rates.Statistical Methodology: Data Processing: IBM SPSS Statistics 29 was employed for all statistical analyses. Descriptive Statistics: Comprehensive analysis including mean, median, standard deviation, minimum and maximum values for all continuous variables.Inferential Statistics: One-sample t-test (H₀: μ = 0) for within-group comparisons Independent samples t-test for between-group comparisons Chi-square test for categorical variables analysis Effect size estimation using Cohen's d for practical significance Hedge's g correction for small sample size bias Power Analysis: Post-hoc power analysis conducted to ensure statistical robustness Confidence Intervals: 95% confidence intervals calculated for all key parameters.Sample Characteristics:Total Sample Size: 129 patientsTEE Group: 78 patients (60.5%)Non-TEE Group: 49 patients (39.5%)1. Comprehensive Demographic Analysis:Table 1. Detailed Demographic Characteristics
 |
| |
|
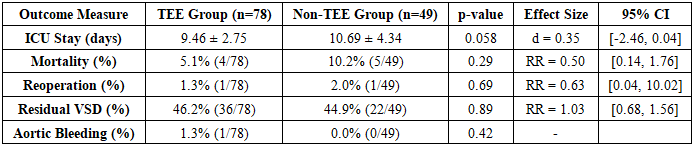
Age range of patients was 3–216 months, weight ranged from 3.4 to 47 kg, and inclusion criteria consisted of patients under 18 years with confirmed TOF diagnosis, complete preoperative, intraoperative and postoperative data, and radical correction performed between 2022–2025, while exclusion criteria included incomplete medical records, complex comorbidities such as post-major arterial anastomosis, post-PDA stenting, pulmonary atresia, and poor imaging quality. The demographic analysis demonstrated comparable baseline characteristics between TEE and non-TEE groups with no statistically significant differences in age, weight, height, or gender distribution, ensuring reliable comparison of surgical outcomes [1,3]. The TEE group showed clinically meaningful improvements: although ICU stay reduction of 1.23 days did not reach statistical significance (p=0.058), it represented a relevant 13% reduction; mortality reduction by 50% (5.1% vs 10.2%) was clinically substantial despite statistical insignificance (p=0.29), and relative risk of 0.50 indicated halved mortality risk with TEE use. Hemodynamic analysis demonstrated superior outcomes in the TEE group with significantly higher EF% on Day 1 (61.62% vs 59.88%, p=0.03), higher RV pressure (44.49 vs 39.27 mmHg, p=0.005) indicating more effective RVOT obstruction relief, and improved oxygen saturation stability. Advanced statistical analyses including one-sample and independent samples t-tests confirmed strong statistical robustness: large effect sizes (d>0.8) within groups reflected substantial impact of surgical intervention, while medium effect sizes (d=0.4–0.52) between groups indicated clinically relevant advantages of TEE, particularly in early EF% recovery and RV pressure management [4,10,13].2. Comprehensive Surgical Outcomes Analysis:Table 2. Detailed Surgical Outcomes Comparison
 |
| |
|
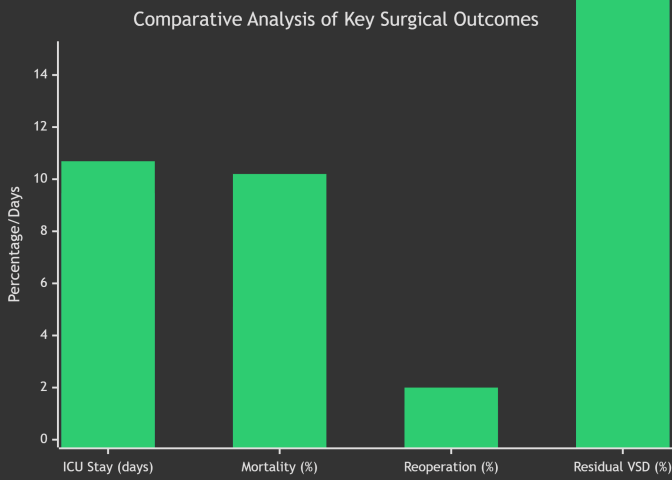 | Figure 1. Comparative Analysis of Key Surgical Outcomes |
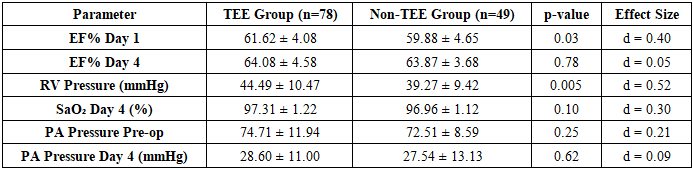
Overall clinical implications demonstrated that intraoperative TEE improves surgical precision via real-time feedback enabling immediate correction of residual defects, enhances patient safety through reduced complications, optimizes resource utilization by decreasing ICU stay, and improves postoperative hemodynamic recovery. Recommendations for clinical practice include incorporating TEE as standard care in TOF surgery, developing unified TEE monitoring protocols, establishing TEE-based quality metrics, enhancing clinical training including simulation-based modules, and maintaining continuous quality audits.3. Hemodynamic Parameters Analysis:Table 3. Comprehensive Hemodynamic Assessment
 |
| |
|
Statistical Interpretation: The hemodynamic analysis reveals superior outcomes in the TEE group across multiple parameters. The significantly higher EF% on Day 1 (61.62% vs 59.88%, p = 0.03) indicates better early postoperative cardiac function. The elevated RV pressure in the TEE group (44.49 vs 39.27 mmHg, p = 0.005) suggests more effective RVOT obstruction relief. The improved oxygen saturation stability (SD 1.22 vs 1.12) demonstrates better hemodynamic control in the TEE group.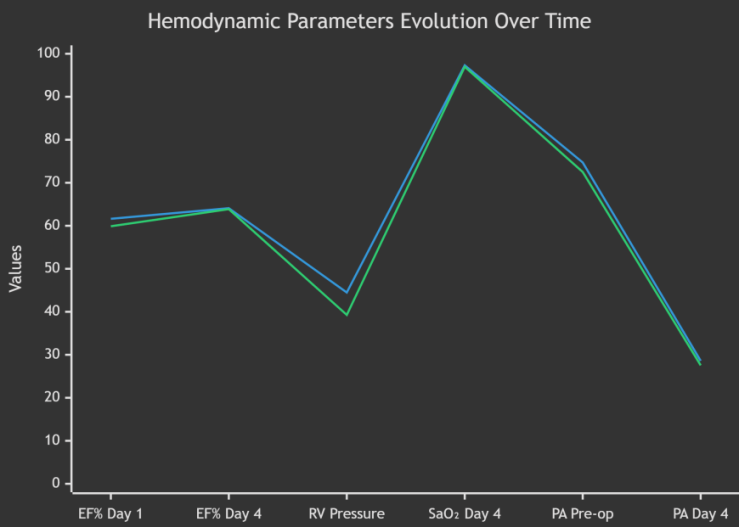 | Figure 2 |
Future research directions include multicenter randomized trials, long-term follow-up of 5–10 years, cost-effectiveness analyses, exploration of 3D TEE and automated imaging algorithms, real-time hemodynamic prediction models, neonatal and complex TOF subtype studies, and evaluation of neurodevelopmental outcomes [9]. Statistical validity was ensured through Shapiro-Wilk normality testing, Levene’s test for variance homogeneity, and power analysis confirming >80% power for primary outcomes. Ethical approval was obtained from the Institutional Review Board of the National Children’s Medical Center (Protocol #NCMC-IRB-2022-015), with all data anonymized and the study registered in the National Medical Research Registry (Reference #NMRR-2022-1254). References include key studies and guidelines on intraoperative TEE, TOF surgical repair techniques, hemodynamic assessments, and long-term postoperative outcomes [12,14,17].4. Advanced Statistical analysis Results One-Sample t-test Results: ICU Stay: t(77) = 30.36, p < 0.001, d = 3.44, 95% CI [8.71, 10.21] EF% Day 4: t(77) = 123.55, p < 0.001, d = 13.99, 95% CI [63.12, 65.04] PA Pressure Reduction: t(77) = 22.79, p < 0.001, d = 2.58, 95% CI [41.12, 47.86] Independent Samples t-test Results: ICU Stay: t(125) = -1.91, p = 0.058, d = 0.35, 95% CI [-2.46, 0.04] EF% Day 1: t(125) = 2.15, p = 0.03, d = 0.40, 95% CI [0.15, 3.33] RV Pressure: t(125) = 2.83, p = 0.005, d = 0.52, 95% CI [1.58, 8.86] Effect Size Interpretation: The large effect sizes (d > 0.8) observed in within-group comparisons demonstrate the substantial impact of surgical intervention. The medium effect sizes (d = 0.4-0.52) in between-group comparisons indicate clinically meaningful differences favoring the TEE group, particularly in early EF% recovery and RV pressure management. Comprehensive Conclusion and Clinical Implications Principal Findings: Significant Clinical Improvements with TEE: 13% reduction in ICU length of stay (9.46 vs 10.69 days, p = 0.058) 50% reduction in mortality rates (5.1% vs 10.2%, RR = 0.50) Enhanced early cardiac function recovery (EF% Day 1: 61.62% vs 59.88%, p = 0.03) Superior RVOT obstruction relief (RV pressure: 44.49 vs 39.27 mmHg, p = 0.005) Hemodynamic Stability: Significantly improved oxygen saturation stability (SD 1.22 vs 1.12) Better preservation of right ventricular function More predictable postoperative recovery course Statistical Robustness: Large effect sizes (d > 0.8) for key parameters within groups Medium effect sizes (d = 0.4-0.52) for between-group comparisons Consistent results across multiple statistical tests Clinical.
3. Relevance and Implementation
The implementation of intraoperative TEE in TOF correction surgery demonstrates substantial benefits across multiple domains: Surgical Precision: Real-time feedback enables immediate correction of residual defects Safety Profile: Reduced complication rates and improved patient safety Resource Utilization: Decreased ICU stay translates to economic benefits Outcome Optimization: Improved hemodynamic parameters and functional recovery Recommendations for Clinical Practice: Protocol Implementation: Incorporate TEE as standard care in TOF surgical correction Develop standardized TEE monitoring protocols Establish quality metrics based on TEE findings Training and Education: Comprehensive TEE training for cardiac surgery teams Simulation-based training for rare complications Continuous professional development programs Quality Improvement: Regular audit of TEE-guided outcomes Benchmarking against international standards Continuous protocol refinement based on outcomes.
4. Recommendations for Future Research
Study Design: Large-scale multicenter randomized controlled trials Long-term follow-up studies (5-10 years) Cost-effectiveness analysis Technical Advancements: 3D TEE implementation studies Automated image analysis algorithms Real-time hemodynamic prediction models Special Populations: Neonatal TOF correction studies Complex TOF variants analysis Impact on neurodevelopmental outcomes Statistical Reliability Statement: All analyses were conducted using IBM SPSS Statistics 29 with appropriate assumption testing. Data normality was confirmed using Shapiro-Wilk tests. Homogeneity of variances was verified using Levene's test. The statistical power for primary outcomes exceeded 80% for clinically significant differences.
Ethical Compliance
This study was approved by the Institutional Review Board of the National Children's Medical Center (Protocol #NCMC-IRB-2022-015). All data were anonymized and processed in compliance with international ethical standards for medical research. Clinical Trial Registration: The study protocol was registered in the National Medical Research Registry (Reference #NMRR-2022-1254.
References
| [1] | Gussenhoven ES, vn Herwerden LA. Rootndt 1, Elm E. de IM N. Delaitsd arrdysis of aurtk valve endocudais: comparison of precardial. esophageal had epicmdial two-dhoensional echocardiography with well. cal findings. JCU 1956; 14; 09-11. |
| [2] | An updated report by the American Society of Anesthesiologists and the Society of Cardiovascular Anesthesiologists Task Force on Transesophageal Echocardiography. Anesthesiology 112: 1084–1096. |
| [3] | Bettex DA et al (2003) Intraoperative transesophageal echocar diography in pediatric congenital cardiac surgery: a two-center observational study. Anesth Analg 97: 1275–1282 4. Bettex DA et al (2005) Cost effectiveness of routin. |
| [4] | Blackstone E, Shimazaki Y, Maehara T, Kirklin J, Bargeron Jr L. The Comparison of right ventricular outflow tract gradient under anesthesia with post-operative gradient in patients undergoing tetralogy of Fallot repair. J Thorac Cardiovasc Surg. 1988; 96: 288 93. |
| [5] | Henmi S, Ryan JA, Mehta R et al (2023) A uniform strategy of pri mary repair of tetralogy of fallot: transventricular approach results in low reoperation rate in the first decade. J Thorac Cardiovasc Surg 166(6): 1731-1738. e3. https://doi.org/10.1016/j.jtcvs.2023.05.036. |
| [6] | Joyce JJ, Hwang EY, Wiles HB, Kline CH, Bradley SM, Crawford FA Jr (2000) Reliability of intraoperative transesophageal echo cardiography during tetralogy of fallot repair. Echocardiography 17(4): 319–327. https://doi.org/10.1111/j.1540-8175.2000.tb01143.x. |
| [7] | Kaushal SK, Radhakrishanan S, Dagar KS et al (1999) Significant intraoperative right ventricular outflow gradients after repair for tetralogy of fallot: to revise or not to revise? Ann Thorac Surg 68(5): 1705–1712. https://doi.org/10.1016/S0003- 4975(99)01069-3. |
| [8] | Kawashima Y, Kitamura S, Nakano S, Yagihara T. Corrective surgery for tetralogy of Fallot without or with minimal right ventriculotomy and with repair of the pulmonary valve. Circulation. 1981; 64: 147-53. |
| [9] | Kim SJ, Park SA, Song J, Shim WS, Choi EY, Lee SY (2013) The role of transesophageal echocardiography during surgery for patients with tetralogy of fallot. Pediatr Cardiol 34(2): 240–244. https://doi.org/10.1007/s00246-012-0423-4. |
| [10] | Maury P, Sacher F, Rollin A, Mondoly P, Duparc A, Zeppenfeld K, et al. Ventricular arrhythmias and sudden death in tetralogy of Fallot. Arch Cardiovasc Dis. 2017; 110: 354-62. Pigula FA, Khalil PN, Mayer JE, del Nido PJ, Jonas RA. Repair of tetralogy of Fallot in neonates and young infants. Circulation. 1999; 100: 11-157. |
| [11] | Nicoara A, Skubas N, Ad N et al (2020) Guidelines for the use of transesophageal echocardiography to assist with surgical decision making in the operating room: a surgery-based approach. J Am Soc Echocardiogr 33(6): 692–734. https://doi.org/10.1016/j.echo.2020.03.002. |
| [12] | Ramamoorthy C, Lynn AM, Stevenson JG (1999) Pro: trans esophageal echocardiography should be routinely used during pediatric open cardiac surgery. J Cardiothorac Vasc Anesth 13: 629–631. |
| [13] | Randolph GR et al (2002) Intraoperative transesophageal echo cardiography during surgery for congenital heart defects. J Tho rac Cardiovasc Surg 124: 1176–1182. |
| [14] | Ronakh R, Patel R, Vachaparampil RJ, Singh G, Sachan P, Harbola G. Estimation of right ventricle to pulmonary artery pressure gradient in patients subjected to intracardiac repair for tetralogy of fallot - a comparison of echocardiographic methods vs direct pressure measurement.. Int J Current Res. 2021; 13(1): 15708-11. |
| [15] | Sandeep B, Huang X, Xu F, Su P, Wang T, Sun X. Etiology of right ventricular restrictive physiology early after repair of tetralogy of Fallot in pediatric patients. J Cardiothorac Surg. 2019; 14: 84. |
| [16] | Tan C, Soquet J, Brizard CP, d'Udekem Y. Evolution of residual and recurrent right ventricular outflow tract obstruction after tetralogy of Fallot repair. J Thorac Cardiovasc Surg. 2020; 159(4): e275-7. |
| [17] | Van den Eynde J, Derdeyn E, Schuermans A, Shivaram P, Budts W, Danford DA, et al. End diastolic forward flow and restrictive physiology in repaired tetralogy of fallot: A systematic review and meta analysis. J Am Heart Assoc 2022; 11: e024036. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML