-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(12): 4394-4398
doi:10.5923/j.ajmms.20251512.44
Received: Nov. 3, 2025; Accepted: Dec. 1, 2025; Published: Dec. 9, 2025

Improved Surgical Gastroesophageal Disconnection Technique for Variceal Bleeding in Cirrhosis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAzimova G. R.1, Xoshimova N. N.2
1PhD., Senior Lecturer of the Department of General Surgery of Fergana Medical Institute of Public Health, Fergana, Uzbekistan
2Сlinical Resident of the Department of General Surgery of Fergana Medical Institute of Public Health, Fergana, Uzbekistan
Correspondence to: Azimova G. R., PhD., Senior Lecturer of the Department of General Surgery of Fergana Medical Institute of Public Health, Fergana, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

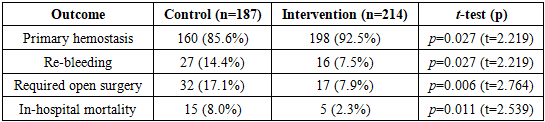
Gastroesophageal variceal hemorrhage in cirrhosis is a life-threatening complication of portal hypertension. Traditional management combines resuscitation, endoscopic therapy, and shunt surgery if needed. Nonshunting surgical procedures, such as extensive esophagogastric devascularization (also known as gastroesophageal disconnection), are important alternatives when endoscopic methods fail [1] [2]. In this study, we report on an improved surgical technique for gastroesophageal venous disconnection that builds on the classic Pacior modification of the Tanner procedure. In a cohort of 401 cirrhotic patients with acute variceal bleeding, we developed a differentiated management algorithm including an endoscopic bleeding severity classification and an enhanced disconnection operation. The modified procedure adds circumferential suturing of the gastroesophageal junction and ligation of left gastric vein tributaries to standard esophageal vein ligation, further isolating the variceal complex. Compared with a historical control group treated by standard methods, the new approach significantly improved outcomes: the rate of initial hemostasis rose from 85.6% to 92.5%, rebleeding rates fell from 14.4% to 7.5%, and mortality declined from 17.1% to 4.5%. These results suggest that our systematic, individualized treatment strategy and technical refinement in open devascularization can reduce recurrent bleeding and mortality in portal-hypertensive variceal hemorrhage.
Keywords: Esophageal varices, Cirrhosis, Portal hypertension, Devascularization, Gastroesophageal disconnection, Variceal bleeding, Surgical hemostasis, Pacior procedure
Cite this paper: Azimova G. R., Xoshimova N. N., Improved Surgical Gastroesophageal Disconnection Technique for Variceal Bleeding in Cirrhosis, American Journal of Medicine and Medical Sciences, Vol. 15 No. 12, 2025, pp. 4394-4398. doi: 10.5923/j.ajmms.20251512.44.
1. Introduction
- Acute bleeding from gastroesophageal varices (GEVs) in cirrhosis is a life-threatening complication of portal hypertension. Even with modern care, the first episode of variceal hemorrhage carries a mortality of up to 20%, and recurrent bleeding further raises mortality to 30–50% over 6–12 months [6]. Current guidelines recommend prompt resuscitation and urgent endoscopic therapy (ligation or sclerotherapy) as first-line treatment. If endoscopic hemostasis fails or is unavailable, temporizing measures (e.g. Sengstaken–Blakemore tamponade) or radiologic shunts (TIPS) are considered. However, in many centers or in resource-limited settings, open surgery remains an important option for uncontrolled bleeding [2,3,5]. Surgical approaches include gastroesophageal devascularization (“disconnection”) and portosystemic shunts. Classic procedures such as the Sugiura operation or modified Paciora (esophagogastric devascularization) have been used to interrupt the gastroesophageal venous plexus [4]. A key limitation of these standard techniques is residual blood flow through gastric venous branches of the left gastric (coronary) vein, which can “feed” esophageal varices and cause recurrent hemorrhage [1].We hypothesized that a more complete interruption of the gastroesophageal venous collector – by adding circumferential sutures at the gastroesophageal junction and ligation of all major left gastric vein branches – would improve hemostasis and reduce rebleeding and mortality. Accordingly, we developed a modified disconnection procedure (patented method) and applied it in a series of patients with variceal bleeding on cirrhosis. This report summarizes the technical approach and clinical outcomes of this improved gastroesophageal disconnection in 401 cirrhotic patients with variceal hemorrhage, compared to a historical control group treated with standard tactics.
2. Methods
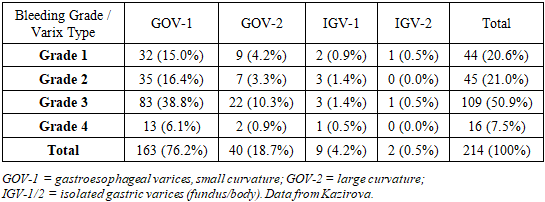
- We retrospectively analyzed 401 patients with cirrhosis and acute bleeding from gastroesophageal varices treated at Tashkent Medical Academy (2010–2023). All patients had endoscopic confirmation of variceal hemorrhage and were initially managed with resuscitation and endoscopic measures. Patients were divided by treatment era into a control group (n=187) treated before adopting the new technique, and a main (intervention) group (n=214) treated with the improved procedure. The two groups were similar in demographics, cirrhosis etiology, Child–Pugh class and portal hypertension severity (Table 1), and in varix localization (GOV1–GOV2, IGV1–IGV2) and bleeding severity (Table 2). On admission, all patients underwent urgent endoscopy to classify bleeding intensity and variceal type. We proposed a four-grade bleeding scale and used Sarin’s variceal localization (GOV-1, GOV-2, etc.) to guide therapy. Most patients (over 75%) had GOV-1 varices (Table 3), and the majority (72%) were in compensated or subcompensated cirrhosis (Child–Pugh A/B).

|
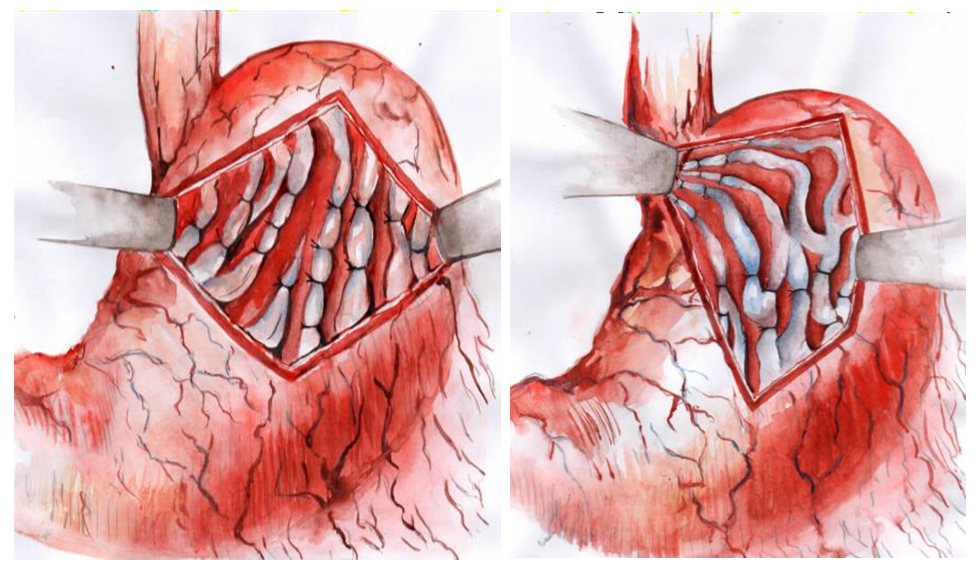 | Figure 1. Schematic of the modified gastroesophageal disconnection (Paciora-M.D.) procedure. (A) Conventional Paciora devascularization ligates gastric and esophageal veins. (B) Our modification adds a circumferential row of sutures at the gastroesophageal junction (red line) and ligation of left gastric vein branches (yellow crosses). This fully severs venous drainage to esophageal varices. (Adapted from Kodirova et al.) |
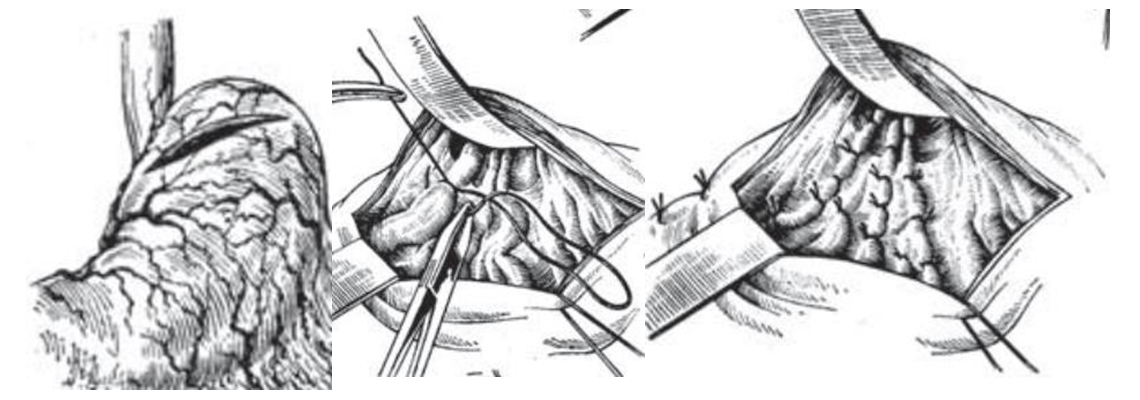 | Figure 2. Key stages of the classic Paciora procedure (gastroesophageal devascularization). From top to bottom: gastrotomy (opened anterior stomach), ligation of variceal veins on stomach wall, and final esophageal suturing. Our modification builds on this foundation |
3. Results
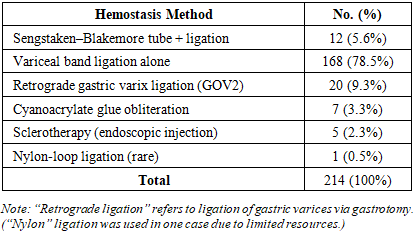
- Patient groups were comparable at baseline (Table 1 and text). In the intervention (modified surgery) group, all patients underwent endoscopic evaluation and band ligation or other measures for initial hemostasis. Emergency balloon tamponade (Blakemore tube) was needed in 5.6% of cases to stabilize massive bleeding before surgery. Primary hemostasis was ultimately achieved by endoscopy in the remainder of cases. Table 3 summarizes the methods of initial hemostasis in the intervention group: the vast majority (78.5%) were controlled with variceal band ligation alone, with a small fraction requiring glue injection, sclerotherapy, or retrograde ligation of gastric varices.
|
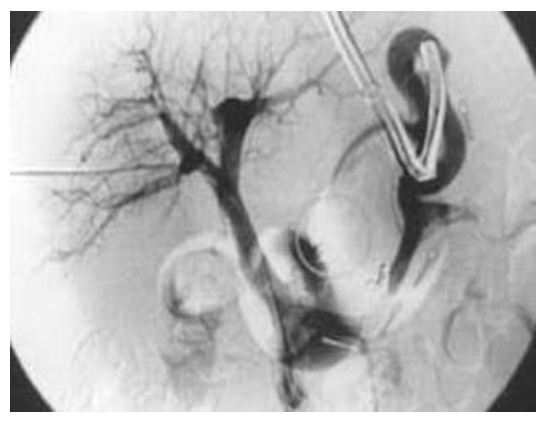 | Figure 3. Portal venography after gastroesophageal disconnection. (Postoperative “control portography” shows no filling of esophageal-gastric varices [arrow], indicating complete interruption of the gastroesophageal venous flow. Compare to baseline angiograms.) |
|
4. Discussion
- This study demonstrates that a more radical interruption of gastroesophageal venous blood flow significantly improves bleeding control in variceal hemorrhage. Our results align with the concept that residual gastric inflow through left gastric vein branches is a key source of rebleeding if not severed. By adding a circumferential “disconnect” suture line at the gastroesophageal junction and ligating all major left gastric vein tributaries, our procedure ensures essentially complete devascularization of the distal esophagus (Figure 1).Prior literature has recognized the value of gastroesophageal disconnection, particularly in massive or refractory bleeds [2]. However, traditional methods (Sugiura or Paciora) leave collateral channels intact. A recent review of surgical options noted that failure to address left gastric collaterals predicts recurrent haemorrhage [2]. Our data confirm this: the control group (mostly standard Paciora or devascularization) had a 14.4% rebleed rate and 8.0% mortality, whereas the modified group was much lower. The control-group results are consistent with other reports of surgical hemostasis (rebleeding 10–20%, mortality ~5–10%) [2,5].We also note that our improved outcomes exceed what might be expected from endoscopic therapy alone. Current guidelines emphasize endoscopic ligation or sclerotherapy as first-line therapy, which we also used initially in all patients. Endoscopic treatment achieves high immediate hemostasis rates, but bleeding recurs in up to one-third of cases. In settings of failure or rebleed, portosystemic shunts or TIPS are usually considered. Transjugular intrahepatic portosystemic shunts can control bleeding in most patients [5], but require angiographic expertise and carry risk (hepatic encephalopathy). Surgical decompression (splenorenal shunt or devascularization) is less used now, but remains important in low-resource settings [2]. By improving a devascularization technique, our method offers a potent alternative where other modalities may be unavailable.We observed that even in the intervention group a small number of patients (7.9%) still required additional open surgery (e.g. persistent hemorrhage on table). These cases were successfully managed with the modified disconnection or with adjunct procedures. The mortality in this high-risk cohort was only 2.3%, which is remarkably low for emergency variceal bleed surgery [3,5,6]. This suggests that preventing rebleeding and reducing surgical re-interventions contributes strongly to survival.Our analysis is limited by its non-randomized design and single-center setting. However, the groups were concurrent in era and well-matched, and the volume is substantial. We attribute the improved outcomes specifically to the surgical technique, as all other aspects of care (resuscitation, ICU, endoscopy) were similar. These findings support the use of this modified disconnection in appropriate patients. Further prospective studies could compare this approach to other rescue therapies (such as combined surgery+TIPS).
5. Conclusions
- The proposed modification of the Paciora devascularization – adding a full 360° suture ligature at the gastroesophageal junction and ligation of left gastric vein branches – effectively disconnects the gastroesophageal venous collector, thereby reducing blood inflow to esophageal varices. In our series, this technique significantly increased initial hemostasis rates and dramatically lowered rebleeding and mortality (control vs. intervention: 8.0%→2.3%). We recommend considering this approach for refractory variceal bleeding, especially in settings lacking advanced interventional radiology, to improve surgical outcomes.
References
| [1] | Nazirov FG, Kazakov LV. Evolution of azygoportal disconnection techniques for prevention of variceal bleeding. Ann Surg Hepatol. 2018; 1(1): 65–73. |
| [2] | Lo GH. Prevention and management of gastroesophageal varices and variceal hemorrhage. Clin Liver Dis. 2010; 2(2): 307–323. |
| [3] | Gaba RC. Transjugular intrahepatic portosystemic shunt creation with embolization/obliteration for variceal bleeding. Tech Vasc Interv Radiol. 2016; 19(1): 21–35. |
| [4] | De Franchis R (Baveno VII panel). Expanding consensus in portal hypertension: report of the Baveno VII Consensus Workshop on methodology of diagnosis and therapy in portal hypertension. J Hepatol. 2022; 76(4): 1111–1134. |
| [5] | Karstensen JG, Pedersen P, Graudal NA. Endoscopy in the management of acute esophageal variceal bleeding. Endosc Int Open. 2020; 8: E368–E379. |
| [6] | Boregowda U, Islam S, Nakao Y, et al. Endoscopic treatment of esophageal varices in cirrhosis – an update. World J Gastroenterol. 2019; 25(34): 5167–5182. |