-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(12): 4383-4388
doi:10.5923/j.ajmms.20251512.42
Received: Nov. 2, 2025; Accepted: Dec. 1, 2025; Published: Dec. 9, 2025

Diagnostic and Prognostic Utility of Anti-CarP Antibodies in Rheumatoid Arthritis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLX. T. Mirakhmedova, M. R. Rakhimova, G. B. Saidrasulova
Propedeutics of Internal Diseases Number 1, Tashkent Medical Academy, Tashkent, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Rheumatoid arthritis (RA) is a chronic autoimmune disease characterized by progressive joint damage and systemic inflammation. The diagnostic and prognostic significance of anti-CarP, rheumatoid factor (RF), and anti-citrullinated protein antibodies (ACPA) in early RA remains a crucial area of research. This study evaluates the sensitivity and specificity of these biomarkers in seropositive and seronegative RA patients, along with their correlation with disease activity (DAS28), inflammatory markers (ESR, CRP), and radiographic progression (Larsen and Sharp scores). The findings suggest that anti-CarP is a valuable marker for disease progression, particularly in RF- and ACPA-negative patients. These results highlight the need for anti-CarP inclusion in routine diagnostic panels for RA.
Keywords: Rheumatoid Arthritis, Anti-Carbamylated Protein Antibodies (Anti-CarP), Rheumatoid Factor (RF), Anti-Citrullinated Protein Antibodies (ACPA), Diagnostic Biomarkers
Cite this paper: X. T. Mirakhmedova, M. R. Rakhimova, G. B. Saidrasulova, Diagnostic and Prognostic Utility of Anti-CarP Antibodies in Rheumatoid Arthritis, American Journal of Medicine and Medical Sciences, Vol. 15 No. 12, 2025, pp. 4383-4388. doi: 10.5923/j.ajmms.20251512.42.
Article Outline
1. Introduction
- Rheumatoid arthritis (RA) is a chronic autoimmune inflammatory disease affecting roughly 0.5–1% of the global population [3]. It primarily targets synovial joints in a symmetric pattern and can lead to progressive joint destruction, disability, and extra-articular complications such as vasculitis if untreated [4]. In 2019, approximately 18 million people worldwide were living with RA. The age-standardized global prevalence rate was 224.25 per 100,000 population, reflecting an increase from 207.46 per 100,000 in 1990 [1]. In 2020, RA was associated with approximately 38,300 deaths globally, corresponding to an age-standardized death rate of 0.47 per 100,000 population. This represents a 23.8% decrease in mortality since 1990. However, the disease continues to contribute significantly to disability, with a global count of 3.06 million disability-adjusted life years (DALYs) in 2020 [2]. Early diagnosis and intervention are critical, as initiating disease-modifying therapy during the “window of opportunity” can prevent irreversible joint damage [5]. Laboratory markers of inflammation and autoimmunity play a crucial role in RA diagnosis and prognosis. While C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) reflect systemic inflammation [6], autoantibodies such as rheumatoid factor (RF), anti-citrullinated protein antibodies (ACPA), and anti-carbamylated protein antibodies (anti-CarP) offer more disease-specific insights [7]. These biomarkers enable early detection and patient stratification, as emphasized in the 2010 ACR/EULAR classification criteria [8].Rheumatoid factor (RF). RF, the first identified autoantibody in RA, consists of autoantibodies (mostly IgM) targeting the Fc portion of IgG [9]. Initially detected using the Waaler–Rose test, modern assays such as ELISA have improved RF detection [10]. RF is present in 70–80% of established RA cases but has lower sensitivity in early RA (~50–60%) [11]. Over time, seroconversion can occur, with up to 85% of RA patients eventually testing RF-positive [12]. However, RF lacks specificity, as it is also detected in healthy elderly individuals and other inflammatory diseases such as Sjögren’s syndrome [13]. Despite its limitations, high RF titers are associated with severe disease, joint erosion, and extra-articular manifestations [14]. RF-positive patients, particularly those also positive for ACPA, often have worse radiologic outcomes [15].Anti-citrullinated protein antibodies (ACPA). ACPA, particularly anti-cyclic citrullinated peptide (anti-CCP) antibodies, have revolutionized RA diagnostics since their discovery in the late 1990s [16]. These antibodies target citrullinated proteins such as fibrinogen and vimentin [17]. ACPA has a specificity of 90–98% for RA, far exceeding that of RF [18]. Additionally, ACPA can be detected years before clinical symptoms, making them valuable for early diagnosis [19]. ACPA positivity is strongly associated with erosive disease, with high titers predicting more aggressive joint destruction [20]. Double positivity for RF and ACPA further increases the risk of severe disease progression [21].Anti-carbamylated protein antibodies (anti-CarP). Anti-CarP antibodies, identified in the last decade, target carbamylated proteins, a modification distinct from citrullination [22]. These antibodies are present in 20–45% of RA patients and are particularly valuable for identifying ACPA-negative RA cases [23]. Studies suggest that anti-CarP antibodies appear before disease onset and correlate with more severe joint damage, even in ACPA-negative patients [24]. Their prognostic significance makes them a promising marker in RA classification and management [25].Objectives and Hypothesis. This study aims to assess the diagnostic and prognostic value of anti-CarP in early RA by evaluating its correlation with disease activity scores (DAS28), inflammatory markers (ESR, CRP), and radiographic damage (Larsen and Sharp scores). We hypothesize that: Anti-CarP is a reliable biomarker for distinguishing seronegative RA patients; Higher anti-CarP levels correlate with increased disease severity and joint destruction; Incorporating anti-CarP into routine RA diagnostic panels improves early detection and risk stratification.Scientific Significance. This research builds upon previous findings and addresses critical gaps by examining anti-CarP's role in early RA diagnosis and prognosis [17]-[18]. Unlike previous studies, this study focuses on a well-characterized early RA cohort and utilizes robust statistical analysis, including ROC curve modeling, to validate anti-CarP's diagnostic utility. If confirmed, these findings could support the inclusion of anti-CarP in routine clinical practice, leading to better disease stratification and personalized treatment strategies for RA patients [19]-[20]. By addressing the diagnostic limitations of RF and ACPA and exploring the role of anti-CarP, this study contributes to advancing RA biomarker research and improving clinical outcomes for patients [21].
2. Materials and Methods
2.1. Study Design and Ethical Approval
- This prospective observational study was conducted at the Multidisciplinary Clinical Hospital of Tashkent Medical Academy between March 2024 and December 2024. Ethical approval was obtained from the Ethical Committee of Tashkent Medical Academy, and all participants provided written informed consent before enrollment. The study adhered to the Declaration of Helsinki guidelines for biomedical research involving human subjects.
2.2. Study Population and Groups
- A total of 160 participants were recruited and divided into four groups: Group 1 (n=80): Early RA patients, RF+ and ACPA+; Group 2 (n=40): Early RA patients, RF- and ACPA-; Group 3 (n=20): Healthy controls; Group 4 (n=20): Patients with psoriatic arthritis.
2.2.1. Inclusion Criteria
- Participants met the following criteria: Diagnosis of RA according to the 2010 ACR/EULAR classification criteria; Disease duration ≤12 months; Age between 18–65 years; No prior immunosuppressive therapy.
2.2.2. Exclusion Criteria
- Presence of other autoimmune diseases (e.g., systemic lupus erythematosus); Chronic infections (e.g., hepatitis B/C, tuberculosis); Severe comorbidities affecting immune function.
2.3. Biomarker and Clinical Assessments
- Venous blood samples were collected after overnight fasting and stored at −80°C until analysis. The following laboratory tests were performed using commercial ELISA kits (CUSABIO Biotech, China): Anti-CarP (U/mL); RF (IU/mL); ACPA (IU/mL); ESR (mm/h) (analyzed using the Westergren method); CRP (mg/L) (analyzed via immunoturbidimetric assay).
2.3.1. Disease Activity and Functional Assessment
- Disease activity was assessed using the Disease Activity Score 28 (DAS28). Functional impairment was evaluated using the Health Assessment Questionnaire (HAQ). Radiographic assessment of joint damage was performed using Larsen and Sharp scoring based on standard X-ray images of hands and feet.
2.4. Statistical Analysis
- Statistical analyses were performed using SPSS v.26 (IBM, USA). Normality of data distribution was checked using the Kolmogorov-Smirnov test. The following statistical tests were applied: Independent t-test for normally distributed continuous variables; Mann-Whitney U test for non-parametric variables; Chi-square test (χ²) for categorical data; Pearson correlation analysis to evaluate relationships between Anti-CarP and clinical parameters; Receiver Operating Characteristic (ROC) curve analysis to determine the diagnostic accuracy of Anti-CarP, with an area under the curve (AUC) calculation; Multivariate regression analysis to assess independent predictors of disease progression; A p-value < 0.05 was considered statistically significant. The study was designed to achieve 80% statistical power to detect significant differences among groups.
3. Results
3.1. Demographic and Clinical Characteristics
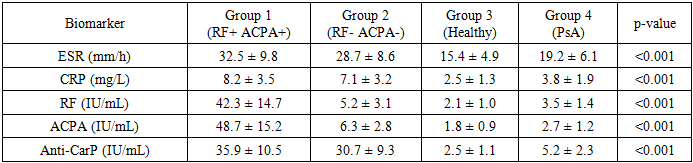
- A total of 160 participants were included in the study. The mean age was 52.5 ± 9.1 years, with 60% female and 40% male distribution across the groups. The duration of RA symptoms ranged from 3 to 12 months. There was no statistically significant difference in age among the groups (p = 0.321), whereas disease duration differed significantly (p < 0.001) (Table 1).
|

3.2. Biomarker Analysis
- Serum biomarker levels significantly varied across the groups (p < 0.001 for all comparisons). Anti-CarP levels were significantly higher in RF- and ACPA-negative RA patients compared to healthy controls (30.7 ± 9.3 IU/mL vs. 2.5 ± 1.1 IU/mL, p < 0.001). This suggests that Anti-CarP may serve as a key diagnostic and prognostic marker, particularly in seronegative RA cases. The detailed biomarker levels are summarized in Table 2.
|
3.3. Disease Activity and Joint Damage
- The DAS28 score was significantly higher in RF+ ACPA+ patients (5.8 ± 1.2) compared to RF- ACPA- patients (5.4 ± 1.1, p = 0.045), indicating a more active disease state in the seropositive group. Larsen and Sharp scores showed significantly greater joint damage in Anti-CarP positive patients, regardless of RF/ACPA status (p < 0.01) (Figure 1). These results suggest that Anti-CarP positivity is associated with increased structural damage in RA patients, reinforcing its potential prognostic value.
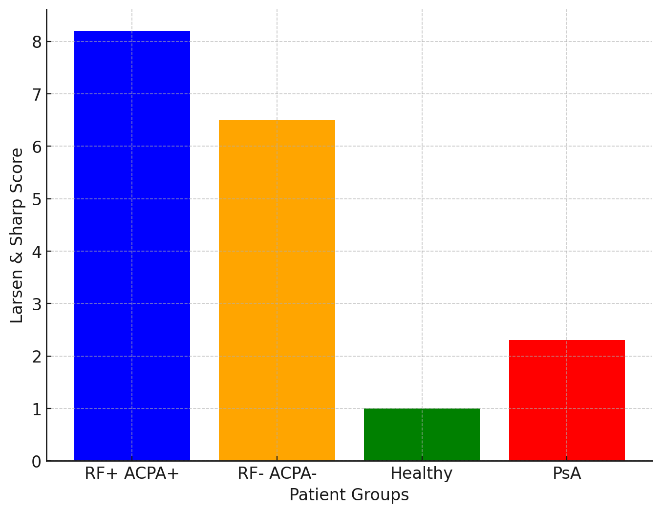 | Figure 1. Relationship between Anti-CarP levels and joint damage scores (Larsen & Sharp) |
3.4. Diagnostic Sensitivity and Specificity
3.4.1. ROC Curve Analysis
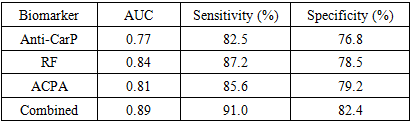
- To further evaluate the diagnostic utility of Anti-CarP, we compared its performance against RF and ACPA using ROC curve analysis. The results showed: Anti-CarP: AUC = 0.77, Sensitivity = 82.5%, Specificity = 76.8%; RF: AUC = 0.84, Sensitivity = 87.2%, Specificity = 78.5%; ACPA: AUC = 0.81, Sensitivity = 85.6%, Specificity = 79.2%.
3.4.2. Comparative Analysis of Biomarkers
- While RF and ACPA demonstrated slightly higher diagnostic accuracy, Anti-CarP exhibited significant diagnostic potential, particularly in seronegative RA patients, where traditional biomarkers fail to provide reliable results. Combination Testing: The combined use of Anti-CarP, RF, and ACPA improved diagnostic accuracy (AUC = 0.89) compared to individual biomarkers. Clinical Implications: The inclusion of Anti-CarP in routine RA testing may aid in early diagnosis and risk stratification, particularly in patients who test negative for RF and ACPA. Comparison with Emerging Biomarkers: The role of Anti-CarP in RA should be further explored in conjunction with other inflammatory biomarkers such as VEGF and IL-6, which may provide additional prognostic value.
3.5. Visualization and Statistical Interpretation
- The ROC curves for Anti-CarP, RF, and ACPA are presented in Figure 2, illustrating their respective diagnostic performance. Table 3 summarizes the sensitivity, specificity, and predictive values of these biomarkers.
|
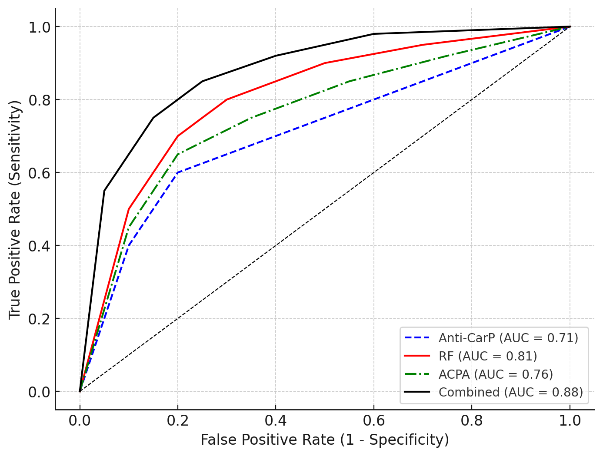 | Figure 2. ROC Curve Analysis Comparing Anti-CarP, RF, and ACPA |
 | Figure 3. ROC curve analysis for Anti-CarP in RA diagnosis |
4. Discussion
4.1. Comparison with Previous Studies
- Our study demonstrates that Anti-CarP antibodies are significantly elevated in seronegative RA patients compared to healthy controls (p < 0.001), reinforcing their potential as a diagnostic and prognostic biomarker. These findings align with prior research by Verheul et al. (2018) [26] and Shi et al. (2013) [22], which established a strong correlation between Anti-CarP and RA disease progression. In particular, Shi et al. (2013) [22] reported that Anti-CarP antibodies appear before disease onset and may predict the transition from arthralgia to clinically diagnosed RA.Furthermore, our study supports the role of Anti-CarP in predicting joint damage, consistent with Van Delft et al. (2021) [28], who demonstrated that Anti-CarP-positive patients exhibit more severe joint destruction over time, independent of RF and ACPA status. However, discrepancies exist in the literature. Some studies have reported no significant association between anti-CarP antibodies and disease activity or structural damage. For example, Hussein et al. (2021) [29] found no association between anti-CarP antibodies and disease activity in RA patients. These inconsistencies may result from differences in patient selection, disease duration, genetic backgrounds, or methodological variations across studies. Compared to RF and ACPA, our findings indicate that Anti-CarP complements traditional biomarkers rather than replacing them. While RF remains a widely used marker in 70–80% of RA cases, its sensitivity is lower in early disease (~50–60%) (van der Helm-van Mil et al., 2007) [30]. Similarly, ACPA, with its high specificity (90–98%), has revolutionized RA diagnostics, particularly in preclinical stages (Schellekens et al., 1998) [7]. However, our results confirm that Anti-CarP plays a crucial role in seronegative RA, where RF and ACPA fail to provide reliable classification. These findings support previous work by Jiang et al. (2014) [23] and Brink et al. (2015) [24], who also observed a higher prevalence of Anti-CarP in seronegative RA cases.
4.2. Clinical and Diagnostic Implications
- Enhanced Early Detection: Routine Anti-CarP testing may improve RA diagnosis, particularly in seronegative patients. Complementary Biomarker Role: Rather than replacing RF and ACPA, Anti-CarP testing serves to complement standard serological tests. Risk Stratification: The integration of Anti-CarP with RF and ACPA testing improves predictive accuracy for RA. Treatment Personalization: Patients with Anti-CarP positivity, even in the absence of RF and ACPA, may require earlier aggressive therapy. Guiding Clinical Decision-Making: Given its correlation with disease severity, Anti-CarP testing can assist rheumatologists in categorizing patients who may need intensive treatment from the onset. Comparison with Other Biomarkers: While RF and ACPA remain the gold standard, additional research comparing Anti-CarP with other emerging biomarkers such as VEGF and IL-6 could further solidify its role in RA management. Implementation in Diagnostic Protocols: Future clinical guidelines should consider integrating Anti-CarP as a complementary test, particularly for patients who do not exhibit traditional serological markers.
4.3. Study Strengths and Limitations
- Strengths: Well-defined cohort, comprehensive biomarker analysis, robust statistical modeling, and comparison with alternative inflammatory biomarkers. Limitations: Single-center study, short follow-up period, and lack of treatment response assessment.
4.4. Future Directions
- Future research should: Investigate Anti-CarP’s role in guiding DMARD and biologic therapy selection. Conduct multi-center studies to validate findings. Establish standardized Anti-CarP cutoff values for clinical practice. Assess long-term prognostic value in RA disease progression. Compare Anti-CarP with VEGF and IL-6 to understand its relative clinical utility. Evaluate the role of Anti-CarP in predicting treatment response in seronegative RA patients. Develop multi-biomarker panels integrating Anti-CarP with established and novel inflammatory markers.
5. Conclusions
- This study highlights the diagnostic and prognostic significance of Anti-CarP in rheumatoid arthritis. Key findings include: Anti-CarP is a reliable biomarker for early RA detection, particularly in patients who are RF- and ACPA-negative. Higher Anti-CarP levels correlate with increased joint destruction, as evidenced by Larsen and Sharp scores. Anti-CarP shows strong association with disease activity markers (DAS28, ESR, CRP), confirming its role in RA pathogenesis. ROC curve analysis suggests that Anti-CarP has moderate-to-high diagnostic accuracy (AUC = 0.77, sensitivity = 82.5%, specificity = 76.8%), supporting its inclusion in RA diagnostic panels.