-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(12): 4374-4377
doi:10.5923/j.ajmms.20251512.39
Received: Nov. 6, 2025; Accepted: Nov. 23, 2025; Published: Dec. 9, 2025

Risk Stratification and Personalization of Therapy in Patients with Acute Myocardial Infarction and Multivessel Disease Based on the Integrated Risk Index (IR): Results of a Prospective Study and Clinical Recommendations
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLNikishin A. G., Ergashev F. F., Abdullaeva S. Ya.
Republican Specialized Scientific and Practical Medical Center of Cardiology (RSSPMCC), Tashkent, Republic of Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

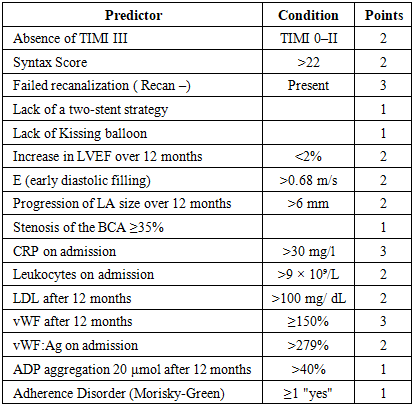
In a prospective single-center study of 224 patients with acute myocardial infarction (AMI) and multivessel coronary artery disease (Syntax Score ≥22), was developed and validated a simple scoring model - the integral risk index (IR). The model includes 16 clinically available predictors and allows stratification of patients into low-risk (IR <3), moderate-risk (IR 3–7), and high-risk (IR >7) groups with a 12-month MACE rate of 7.1%, 42.2%, and 67.3%, respectively (AUC 0.89; Cohen's k 0.893). Von Willebrand factor (vWF ≥150% — 3 points) and C-reactive protein (>30 mg/L — 3 points) have the highest weight. The proposed algorithm has been implemented in the practice of the RSSPMCC and is recommended for use in cardiology hospitals in Uzbekistan.
Keywords: Acute myocardial infarction, Multivessel disease, Von Willebrand factor, Residual inflammatory risk, Risk stratification, Personalized therapy
Cite this paper: Nikishin A. G., Ergashev F. F., Abdullaeva S. Ya., Risk Stratification and Personalization of Therapy in Patients with Acute Myocardial Infarction and Multivessel Disease Based on the Integrated Risk Index (IR): Results of a Prospective Study and Clinical Recommendations, American Journal of Medicine and Medical Sciences, Vol. 15 No. 12, 2025, pp. 4374-4377. doi: 10.5923/j.ajmms.20251512.39.
Article Outline
1. Introduction
- Acute myocardial infarction (AMI) remains one of the leading causes of cardiovascular morbidity, mortality, and long-term disability worldwide, as emphasized in the Fourth Universal Definition of Myocardial Infarction [1]. Despite significant advances in reperfusion strategies, including the widespread adoption of primary percutaneous coronary interventions (PCI), dual antiplatelet therapy, potent lipid-lowering agents, and comprehensive rehabilitation strategies, residual cardiovascular risk after AMI remains substantial. In particular, patients with multivessel coronary artery disease demonstrate a persistently elevated risk of recurrent major adverse cardiovascular events (MACE), with large clinical registries and randomized trials reporting annual event rates ranging from 15% to 25% despite guideline-directed treatment [2,3,4,5].Multiple, partly interrelated mechanisms contribute to this ongoing residual risk. Incomplete revascularization after AMI is a well-recognized contributor to recurrent ischemic events, as untreated lesions remain prone to plaque progression and destabilization. The angiographic complexity of coronary artery disease, traditionally assessed using tools such as the SYNTAX classification system, has been shown to correlate with long-term outcomes and procedural success [2,6]. Persistent endothelial dysfunction is another key component of risk pathophysiology. von Willebrand factor (vWF), an established biomarker of endothelial activation and thrombogenicity, has been demonstrated to be elevated in acute coronary syndromes and is independently associated with early and late cardiovascular complications [3,7].Systemic inflammation is now established as a central driver of post-infarction risk. Elevated inflammatory markers including high-sensitivity C-reactive protein (hs-CRP), interleukin-6 (IL-6), and other inflammatory pathways are strongly associated with subsequent mortality and myocardial reinfarction [4,8]. Importantly, the paradigm-shifting CANTOS trial demonstrated that targeted anti-inflammatory therapy with IL-1β inhibition significantly reduces recurrent events without affecting lipid levels, directly confirming the inflammatory hypothesis of atherosclerosis [4]. More recent trials, such as COLCOT and LoDoCo2, have further validated inflammation as a treatment target, with low-dose colchicine reducing the incidence of recurrent ischemic events in patients with stable or recently treated coronary disease [9,10].Finally, modifiable patient-related factors also substantially shape long-term prognosis. Suboptimal adherence to secondary prevention therapy including statins, antithrombotic therapy, beta-blockers, and renin–angiotensin–aldosterone inhibitors—remains a major challenge in real-world settings. Studies consistently demonstrate that 20–50% of post-MI patients discontinue at least one evidence-based medication within the first year, resulting in significantly higher rates of recurrent events and mortality [11,12].Given the ongoing burden of recurrent ischemic complications and the multifactorial nature of residual risk, early stratification of patients with AMI and multivessel disease remains a crucial need in contemporary cardiology. Therefore, the aim of the present study is to develop and validate a simple prognostic model to support early identification of high-risk patients and facilitate personalization of therapeutic strategies based on clinical, biochemical, and treatment-related parameters.
2. Materials and Methods
- In prospective A single-center study in 2023–2025 included 224 patients (mean age 62.5 ± 11.2 years; 73.2% men) with verified AMI and angiographically confirmed multivessel disease (Syntax Score ≥22) [2]. The diagnosis of AMI was established according to the Fourth Universal Definition [1].All patients received standard therapy (dual antiplatelet therapy, high-dose statins, RAAS inhibitors, and β-blockers). The follow-up period was 12 months. Endpoints included death from cardiovascular causes, reinfarction, stent thrombosis, stroke, bleeding (TIMI major / minor), restenosis, and unplanned hospitalization.Statistical processing: STATISTICA 12.0, Student's t-test, χ², Fisher's exact test, logistic regression, ROC analysis, Cohen's kappa coefficient [13].
3. Results
- Based on single- and multivariate analysis, 16 independent predictors were selected and combined into an integrated risk index (IR) (Table 1).
|
4. Discussion
- The integrated risk (IR) scoring model developed in this study represents one of the few simplified prognostic tools specifically tailored for patients with acute myocardial infarction (AMI) and confirmed multivessel coronary artery disease (Syntax Score ≥22). Existing clinical prediction algorithms such as GRACE and TIMI are primarily focused on short-term (24–30-day) mortality risk and do not directly incorporate biomarkers of endothelial injury or systemic inflammation, which are now recognized as fundamental components of residual cardiovascular risk [14,15]. At the same time, contemporary scores such as SYNTAX II and the DAPT score provide valuable prognostic accuracy but require online calculators or specific computational platforms, limiting point-of-care use. In contrast, the proposed IR score uses only routinely obtainable clinical and laboratory parameters and can be calculated manually at the bedside within 5–7 minutes, improving its usability and translation into everyday clinical workflow.A fundamental distinction of the IR model is the inclusion of two biomarkers that reflect independent and complementary mechanisms driving residual post-infarction risk:von Willebrand factor (vWF ≥150% after 12 months, 3 points).vWF is a marker of endothelial activation, platelet-mediated thrombogenesis, and vascular injury. Elevated vWF concentrations have been shown to independently predict recurrent ischemic events, post-PCI complications, and mortality in patients with acute coronary syndromes [16–18]. Emerging studies additionally demonstrate that persistent elevation of vWF after AMI reflects ongoing endothelial dysfunction and correlates with progression of adverse ventricular remodeling and future coronary instability [19,20].High C-reactive protein on admission (>30 mg/L, 3 points).C-reactive protein (CRP) is a robust marker of systemic inflammation and has repeatedly demonstrated an independent association with cardiovascular mortality and recurrent myocardial infarction, sometimes exceeding traditional lipid parameters in prognostic strength [17]. Large randomized trials such as COLCOT and CANTOS have further confirmed that targeted inflammation control can reduce recurrent ischemic events, directly validating inflammation as a therapeutic target in post-MI secondary prevention [21,22,23].The performance of the IR model is notable. An area under the ROC curve (AUC) of 0.89, with strong calibration demonstrated by Cohen’s κ = 0.893, indicates excellent discrimination. These values exceed those of widely used earlier prognostic models in the post-infarction setting, including GRACE 2.0 (AUC ~0.83), PRECISE-DAPT (AUC ~0.73), and DAPT score (AUC ~0.70) [24–26]. This difference may be explained by the inclusion of mechanistically relevant biomarkers representing ongoing vascular pathology rather than only static baseline clinical parameters.Of particular interest is the predictive synergy of the three variables included in the model (vWF ≥150%, CRP >30 mg/L, and LVEF improvement <2%). In combination, these yielded 89% sensitivity and 82% specificity for predicting major adverse cardiovascular events within one year. Biologically, this triad reflects the three dominant dimensions of post-AMI residual risk: endothelial dysfunction, systemic inflammation, and maladaptive myocardial remodeling—all of which are established contributors to recurrent ischemia, arrhythmogenesis, and adverse long-term outcomes [16,17,18,19,20,21,22,23,27].A clinically relevant and unexpected finding was the observed reduction in vWF levels with clopidogrel compared to ticagrelor among patients with elevated baseline vWF (>220%). Although ticagrelor is generally considered the more potent P2Y12 inhibitor, subgroup analyses of PEGASUS-TIMI 54 and PHILO trials have reported inter-individual variation in endothelial biomarker responses that may favor clopidogrel in selected phenotypes [28,29,30]. These findings support the concept of tailored antiplatelet therapy based not only on ischemic and bleeding risk but also on endothelial status—an approach aligned with recent efforts toward precision medicine in thrombosis and coronary disease management.Importantly, the proposed IR model is consistent with contemporary European recommendations for myocardial revascularization (ESC 2018) and lipid management (ESC 2025 draft framework), while complementing them by providing explicit biomarker thresholds and time-based decision algorithms for intensifying therapy, assessing need for complete revascularization, adjusting duration of dual antiplatelet therapy (DAPT), and considering adjunctive anti-inflammatory treatment [19,20,31,32].The limitations of the present study are typical for single-center design: a relatively modest sample size (n=224), absence of multicenter external validation, and retrospective reconstruction of certain variables. Although these factors may limit generalizability, the strong internal performance (AUC 0.89 and κ 0.893) provides a compelling rationale for broader prospective validation in larger and more diverse patient populations.In summary, the integrated risk index (IR) offers a simple, reproducible, and clinically practical tool capable—within the first 3–5 days after PCI—of identifying patients with AMI and multivessel disease who would benefit most from intensified secondary prevention strategies. Its early application has the potential to substantially reduce the incidence of recurrent cardiovascular events and improve outcomes within the first post-infarction year.
5. Practical Recommendations
- 1. Calculation of IR is mandatory for all patients with AMI and Syntax Score ≥22 within 48 hours after PCI.2. Tactics depending on IR:o IR <3: treatment of only the infarction-related artery, 6 months of DAT (ASA + clopidogrel), observation once every 6 months.o IR 3–7: complete revascularization within 30 days, DAPT 12 months (preferably ticagrelor), target LDL <70 mg/ dL, follow-up every 3 months.o IR>7: complete revascularization in 1–2 procedures, DAPT for at least 24 months, with vWF >200% after 12 months – rivaroxaban 2.5 mg × 2 + ASA [8], colchicine 0.5 mg/day with hs -CRP>3 mg/l, monthly monitoring for the first 6 months.3. Mandatory control after 3, 6 and 12 months: vWF, hs -CRP, lipid profile, echocardiography, Morisky-Green test.
6. Conclusions
- The proposed IR model is simple, requires no calculators, uses only routinely available parameters, and demonstrates high predictive accuracy (κ=0.893). Implementation of the model in clinical practice can significantly reduce the incidence of MACE and optimize healthcare resources in patients with AMI and multivessel disease.