-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(12): 4371-4373
doi:10.5923/j.ajmms.20251512.38
Received: Nov. 7, 2025; Accepted: Nov. 25, 2025; Published: Dec. 9, 2025

Prognostic and Preventive Approaches in Complicated Odontogenic Inflammatory Diseases
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAbdullaev Sh. Y.1, Babokhujaev A. S.2
1Doctor of Medical Sciences, Professor, Tashkent State Medical University, Tashkent, Uzbekistan
2Researcher, Tashkent State Medical University, Tashkent, Uzbekistan
Correspondence to: Abdullaev Sh. Y., Doctor of Medical Sciences, Professor, Tashkent State Medical University, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The article summarizes the results of a clinical study that included 91 patients with complicated odontogenic inflammatory diseases (OID). Expanded data of clinical-laboratory analysis, immunological indicators, and features of microbiological and morphometric changes of the wound process are presented. Based on the obtained data, a prognostic algorithm and a preventive scheme were developed, allowing a reduction in the incidence of multiple organ failure and an improvement in treatment outcomes.
Keywords: Odontogenic inflammatory diseases, SOFA, AIDOS, SIRS
Cite this paper: Abdullaev Sh. Y., Babokhujaev A. S., Prognostic and Preventive Approaches in Complicated Odontogenic Inflammatory Diseases, American Journal of Medicine and Medical Sciences, Vol. 15 No. 12, 2025, pp. 4371-4373. doi: 10.5923/j.ajmms.20251512.38.
1. Introduction
- Odontogenic inflammatory diseases represent a significant clinical challenge due to their rapid progression, anatomical complexity, and high risk of severe systemic complications. In many cases, infections that originate from dental or periodontal structures spread through the fascial spaces of the maxillofacial region, leading to extensive purulent-necrotic involvement. When left untreated or inadequately managed, these infections may progress to systemic inflammatory response syndrome (SIRS), sepsis, and multiple organ dysfunction syndrome (MODS), posing a serious threat to patient survival [1]. The severity of odontogenic infections is largely determined by a combination of clinical, immunological, and microbiological factors. Recent studies have demonstrated that pro-inflammatory cytokines such as interleukin-1β (IL-1β), interleukin-6 (IL-6), interleukin-8 (IL-8), and tumor necrosis factor-alpha (TNF-α) play a pivotal role in the development and progression of systemic complications. Elevated levels of these cytokines reflect the intensity of the immune response and correlate with worsening clinical status, including deterioration in organ function assessed by the SOFA scoring system. Despite advancements in antimicrobial therapy and surgical treatment techniques, the incidence of severe complications remains significant. This highlights the urgent need for reliable prognostic tools capable of identifying high-risk patients at an early stage. Early recognition of unfavorable immune and biochemical markers may contribute to the timely initiation of targeted therapeutic strategies, improving treatment outcomes and reducing mortality [5,6].Therefore, the development of an evidence-based prognostic algorithm integrating immunological predictors, clinical criteria, and laboratory markers is essential. Such an approach may provide clinicians with an objective foundation for evaluating disease severity, anticipating complications, and optimizing patient management in cases of complicated odontogenic infections [2,4,7].Purpose of study. Optimization of prognosis and prevention of complications of OID through analysis of clinical, laboratory, immunological, morphometric, and microbiological indicators.
2. Materials and Methods
- The study included 91 patients with OID complicated by infection generalization. The control group consisted of 44 patients, the main group - 47. Patients underwent a comprehensive examination: clinical, laboratory (CRP, PCT, LIS, GPI), immunological (IL-1β, IL-6, IL-8, TNF-α), microbiological (species composition and quantity of microorganisms), morphometric (structure of the wound infiltrate). Severity of condition was assessed using SOFA and “Sepsis-3” criteria.
3. Results and Discussion
- The clinical picture in most patients was characterized by pronounced intoxication, an increase in body temperature up to 38.5±0.6 °C, trismus (61.5% of cases), dysphagia (46.1%), limitation of tongue mobility, and swelling of the oropharynx. The average time from disease onset to hospitalization was 8.2±2.1 days, which contributed to the development of widespread phlegmons.Signs of systemic inflammatory response (SIRS) were observed in 76% of patients. In 32% there was an increase in SOFA ≥ 2 points, which corresponded to the criteria of sepsis according to “Sepsis-3.” The respiratory organs were most often affected (69%), the cardiovascular system (54%), less often the kidneys and liver (22% and 17%, respectively). Levels of pro-inflammatory cytokines were significantly elevated. IL-8 and TNF-α demonstrated the strongest association with severity of condition. The correlation analysis confirmed a significant direct association between IL‑8 levels and SOFA score. Higher IL‑8 concentrations corresponded to increased systemic severity (pic-1). Their concentrations correlated with the extent of involvement of cellular spaces and the severity of organ dysfunction. CRP and PCT markers showed significant prognostic value: in patients with subsequent multiple organ failure, CRP exceeded normal values by 9–11 times, PCT - by 6–8 times.
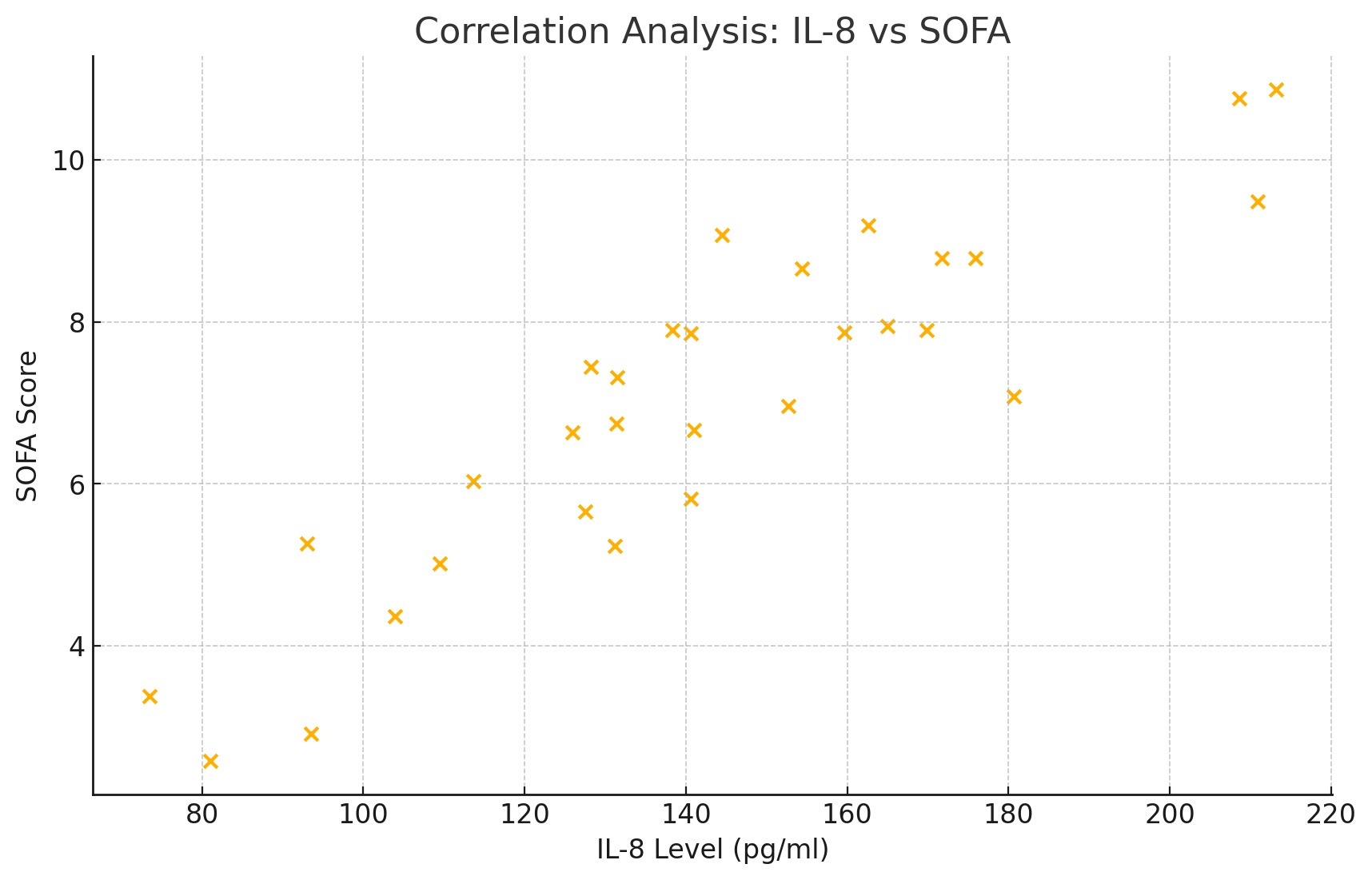 | Picture 1. Correlation analysis: between IL-8 SOFA |
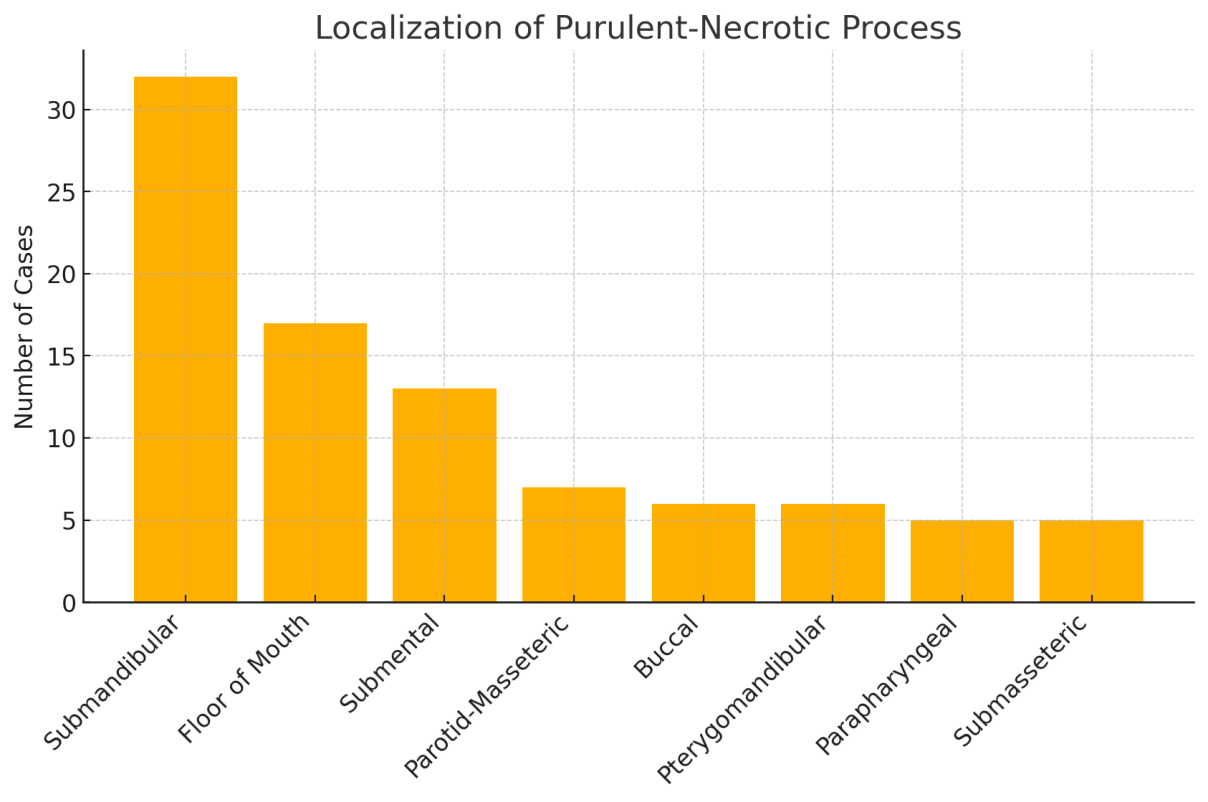 | Picture 2. Localization of purulent – necrotic process |
4. Conclusions
- The conducted study demonstrates that the integration of immunological, microbiological, clinical, and morphometric parameters significantly enhances the accuracy of predicting complications in patients with complicated odontogenic inflammatory diseases. Early identification of patients at high risk using the AIDOS prognostic algorithm enables timely preventive interventions, reducing the incidence of multiple organ failure and improving clinical outcomes. The results support the importance of a comprehensive diagnostic and preventive strategy to optimize treatment efficiency and reduce hospitalization duration in this patient population.