-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(12): 4368-4370
doi:10.5923/j.ajmms.20251512.37
Received: Nov. 8, 2025; Accepted: Nov. 30, 2025; Published: Dec. 9, 2025

Comparative Assessment of the Clinical Effectiveness of Ursodeoxycholic and Obeticholic Acids in Drug Therapy of Patients with Metabolically Associated Fatty Liver Disease
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKarimov M. M.1, Abdullaeva U. K.2, Nurullaeva D. F.3
1Republican Specialized Scientific and Practical Medical Center of Therapy and Medical Rehabilitation, Uzbekistan
2Bukhara State Medical Institute, Uzbekistan
3Bukhara Regional Multidisciplinary Medical Center, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The results of a comparative study on the effectiveness of ursodeoxycholic and obeticholic acids in metabolically associated fatty liver disease at the stage of steatohepatitis are presented. The first group of patients received only ursodeoxycholic acid. The second group of patients, who demonstrated ursoresistance, received only obeticholic acid. In the third group of patients, a combination of ursodeoxycholic and obeticholic acids was used. In the monotherapy regimen, the effectiveness of ursodeoxycholic acid in relation to cytolysis was 10.3% higher for alanine aminotransferase levels and 5.2% higher for aspartate aminotransferase levels (p < 0.05) compared to obeticholic acid. When ursodeoxycholic and obeticholic acids were combined, the hepatoprotective effect was potentiated. Regarding the HOMA IR indicator, the effectiveness of obeticholic acid was 0.7% higher (p<0.05) compared to ursodeoxycholic acid.
Keywords: Obeticholic acid, Ursodeoxycholic acid, Metabolically associated fatty liver disease, Insulin resistance
Cite this paper: Karimov M. M., Abdullaeva U. K., Nurullaeva D. F., Comparative Assessment of the Clinical Effectiveness of Ursodeoxycholic and Obeticholic Acids in Drug Therapy of Patients with Metabolically Associated Fatty Liver Disease, American Journal of Medicine and Medical Sciences, Vol. 15 No. 12, 2025, pp. 4368-4370. doi: 10.5923/j.ajmms.20251512.37.
1. Introduction
- In terms of frequency, non-alcoholic fatty liver disease (NAFLD) has traditionally occupied a leading position among hepatobiliary system diseases in recent decades due to the global trend towards obesity. Global statistics confirm that the prevalence of NAFLD has a clear trend towards an increase in the number of patients in this group. However, the lack of clear criteria for diagnosing and screening NAFLD makes it difficult to develop clear mechanisms for early diagnosis, drug therapy, and prevention of this pathology. This, in turn, led to a revision of the approach to defining the disease itself and renaming the term NAFLD to metabolically associated fatty liver disease (MAFLD) [1]. By definition, MAFLD is a chronic disease characterized by increased fat accumulation in the liver, based on metabolic dysfunction. The basis for diagnosing MAFLD is the presence of liver steatosis in combination with one of the following criteria: high body mass index, presence of type 2 diabetes mellitus, or metabolic dysregulation [3]. In this regard, the main focus of complex therapy in the treatment of MAFLD should be directed both at improving hepatocyte function and at correcting insulin resistance and body weight. According to EASL, EASD, and EASO recommendations, in patients with MAFLD with purely hepatic steatosis, dietary recommendations and adequate physical activity recommendations, even without prescribing medications, are a basic tactic [2]. The use of drugs should be aimed at correcting the function of hepatocytes, insulin resistance, and other comorbid conditions. Unfortunately, the arsenal of drugs used in the treatment of this pathology remains traditional, including pharmacological substances that increase tissue sensitivity to insulin, statins (in the presence of hyperlipidemia), ursodeoxycholic acid (UDCA), and vitamin E. The new recommended drugs used in MAFLD include obeticholic acid (OCA) - an agonist of FXR farnesoid receptors (a drug called REGENERATE). Other FXR agonists (tropifexor, cilofexor, etc.) can also be beneficial for MAFLD [7]. The results of a number of randomized studies showed that OCA contributes to the reduction of inflammatory processes in hepatocytes and the fibrosis process [6]. FXR is a regulator of a large number of genes responsible for bile acid synthesis and transport, lipid metabolism, and glucose homeostasis [9]. FXR controls glucose metabolism and glycogenolysis in the liver, and insulin sensitivity in peripheral tissues. At the same time, it is believed that OCA reduces insulin resistance and normalizes liver inflammation in patients with type 2 diabetes mellitus and MAFLD [4]. Indications for the use of OCA in various stages of MAFLD are discussed, with recommended doses of this drug ranging from 5 to 25 mg per day, which creates certain problems in prescribing this pharmacological substance for MAFLD [4].The aim of this study was to conduct a comparative evaluation of the hepatoprotective effect of OCA versus UDCA in patients with MAFLD associated with insulin resistance. We also assessed the effectiveness of OCA in patients resistant to UDCA and the combination of OCA with UDCA.
2. Material and Methods
- 112 patients with a verified diagnosis of MAFLD associated with insulin resistance were examined: 58 men and 54 women aged 26 to 64 years. Patients with MAFLD were divided into 4 comparable groups according to gender, age, clinical course features, and biochemical indicators of cytolysis and cholestasis. The first group of patients received ursodeoxycholic acid (UDCA) orally at a dose of 12-15 mg/kg for 3 months. The second group of patients consisted of those with UDCA resistance, in whom the previous administration of UDCA at a dose of 12-15 mg/kg had no significant effect (n=18), or with individual intolerance to UDCA in the form of dyspeptic disorders or diarrhea (n=20). Additionally, four patients from this group refused UDCA due to the presence of an intact gallstone. Patients of this group received oral obeticholic acid (OCA) at a dose of 5 mg for 3 months. Finally, the third group of patients received a combination of UDCA at a dose of 12-15 mg/kg and OCA orally at a dose of 5 mg for 3 months. Repeated biochemical control was carried out after 3 months. The activity of aminotransferases (ALT, AST), bilirubin levels, alkaline phosphatase (ALP), and gamma-glutamyltranspeptidase (GGT) was assessed. The level of insulin resistance was evaluated using the HOMA index. All data obtained during the study were entered into Excel summary tables. Dynamic comparison was carried out using Student's paired t-test. Intergroup comparison of indicators was carried out using the unpaired Student's t-test.
3. Results and Discussion
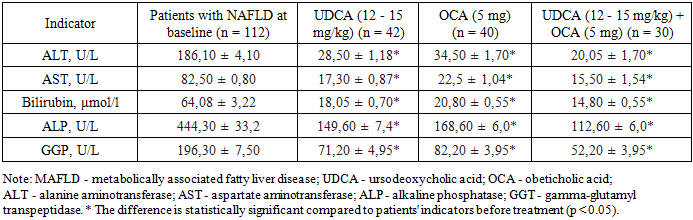
- Preliminary analysis of cytolysis and cholestasis indicators in the examined patients with NAFLD showed that the disease stage, according to the dichotomy, corresponded to the stage of non-alcoholic steatohepatitis (NASH). In the first group of patients, the administration of UDCA at a dose of 12-15 mg/kg for 3 months led to a decrease in ALT activity by 84.5% and AST activity by 79.1% (p < 0.05) (Table 1). Cholestasis indicators in these patients also decreased: bilirubin levels by 71.8%, ALP by 66.3%, and GGT by 73.7% (p < 0.05), respectively. In the second group of patients with NASH who received OCA at a dose of 5 mg for 3 months, we also observed a decrease in cytolysis and cholestasis indicators. ALT and AST levels in this group of patients decreased by 81.5% and 82.7% (p < 0.05), respectively.
|
|

4. Conclusions
- Thus, the obtained results indicate that in terms of hepatoprotective activity, UDCA has advantages over OCA in MAFLD, and in the treatment of patients with steatohepatitis, UDCA is the drug of choice. However, if it is not possible to use UDCA in patients for various reasons, OCA monotherapy is advisable. The combination of UDCA and OCA in patients with steatohepatitis can be justified in cases of MAFLD comorbidity with insulin resistance, or for the mutual enhancement of hepatoprotective effects. At the same time, further research is needed to determine the most effective and safe doses and timeframes for using OCA in the treatment of patients with MAFLD. It can also be concluded that further research into the effects of OCA is promising both for scientific research and for clinical practice.