-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(12): 4360-4363
doi:10.5923/j.ajmms.20251512.35
Received: Oct. 26, 2025; Accepted: Nov. 22, 2025; Published: Dec. 8, 2025

Optimization of Prevention and Treatment Methods for Menstrual Cycle Disorders in Adolescent Girls
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLF. N. Sabirov
PhD, Assistant, Tashkent State Medical University, Tashkent, Uzbekistan
Correspondence to: F. N. Sabirov, PhD, Assistant, Tashkent State Medical University, Tashkent, Uzbekistan.
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Menstrual cycle disorders are among the most frequent gynecologic problems in adolescent girls and often reflect the functional immaturity of the hypothalamic–pituitary–ovarian axis, endocrine instability, nutritional deficiencies, stress-related dysfunction, or metabolic imbalance. Effective prevention and treatment require early recognition of risk factors, comprehensive assessment, and individualized intervention strategies. This study presents an integrated clinical approach aimed at optimizing preventive measures and therapeutic methods for adolescents with menstrual irregularities. A total of over five hundred adolescent patients with various cycle disturbances—including oligomenorrhea, amenorrhea, anovulatory cycles, and dysfunctional uterine bleeding—were clinically evaluated. Diagnostic work included hormonal profiling, pelvic ultrasonography, assessment of metabolic status, and evaluation of psychosocial and lifestyle factors. Preventive strategies focused on menstrual education, nutritional correction, physical activity counseling, and stress-reduction programs. Treatment approaches included hormonal regulation (cyclic progestins or combined therapy), metabolic correction when indicated, and targeted management of contributing factors such as weight fluctuation, sleep disruption, or emotional stress. Analysis showed that structured preventive programs significantly reduced the frequency and severity of menstrual disturbances, while individualized treatment improved cycle stability, hormonal profiles, and overall well-being. The findings highlight the necessity of a combined approach that integrates physiological, behavioral, and educational components for the optimal management of menstrual cycle disorders in adolescent girls.
Keywords: Adolescent gynecology, Menstrual cycle disorders, Anovulation, Cycle regulation, Hormonal imbalance, Preventive strategies, Lifestyle modification, Reproductive health promotion, Psychosocial factors, Metabolic contributors
Cite this paper: F. N. Sabirov, Optimization of Prevention and Treatment Methods for Menstrual Cycle Disorders in Adolescent Girls, American Journal of Medicine and Medical Sciences, Vol. 15 No. 12, 2025, pp. 4360-4363. doi: 10.5923/j.ajmms.20251512.35.
1. Introduction
- Menstrual cycle disorders in adolescent girls represent one of the most common challenges in pediatric and adolescent gynecology. During puberty, the hypothalamic–pituitary–ovarian (HPO) axis undergoes gradual maturation, making adolescents especially vulnerable to cycle instability, anovulation, hormonal fluctuations, and irregular endometrial responses. While many disturbances are functional and self-limiting, a significant proportion require structured preventive strategies and targeted medical intervention due to their association with metabolic imbalance, emotional stress, nutritional deficiencies, and lifestyle-related factors [1]. Adolescents frequently present with oligomenorrhea, amenorrhea, dysfunctional uterine bleeding, or irregular ovulatory patterns. These conditions not only affect reproductive health but may also impair psychological well-being, physical development, school performance, and long-term fertility potential. Studies have shown that up to one-third of adolescent girls experience clinically significant menstrual irregularities requiring medical evaluation, and a substantial number benefit from early preventive interventions aimed at stabilizing hormonal function and modifying risk factors [2]. Effective management relies on a multidimensional approach. Preventive strategies include menstrual education, optimizing body weight, balancing nutrition, promoting regular physical activity, and addressing psychosocial stressors that often contribute to hypothalamic dysfunction. Clinical evaluation typically combines hormonal profiling, pelvic ultrasonography, metabolic screening, and lifestyle assessment. Therapeutic interventions are selected individually and may include cyclic progestin support, combined hormonal regulation, correction of metabolic abnormalities, and behavioral or stress-reduction techniques [3].Despite the availability of these strategies, many adolescents do not receive adequate guidance or timely treatment, highlighting the need for optimized, integrated models of prevention and therapy. This study focuses on identifying effective approaches that combine physiological, behavioral, and educational components to improve menstrual health outcomes in adolescent girls.
2. Materials and Methods
- This study was conducted as a clinical-analytical observational project involving adolescent girls aged 12 to 18 years presenting with various menstrual cycle disorders. A total of over five hundred adolescents were examined as part of a comprehensive reproductive health program. Participants were evaluated following standardized adolescent gynecology protocols, and inclusion criteria comprised oligomenorrhea, secondary amenorrhea, anovulatory cycles, dysovulatory patterns, or dysfunctional uterine bleeding.Exclusion criteria included known congenital reproductive anomalies, diagnosed endocrine tumors, chronic systemic illness, or ongoing hormonal therapy. A comparative reference group of healthy adolescents with regular menstrual cycles was used to define expected physiological ranges for hormonal and ultrasonographic parameters. All participants underwent a structured medical evaluation consisting of:• Detailed menstrual history (cycle length, flow pattern, onset of irregularities)• Anthropometric measurements (BMI, growth velocity, body composition trends)• Evaluation of nutritional habits and physical activity• Screening for stress, sleep patterns, and psychosocial factors• Assessment of symptoms suggestive of hypothalamic dysfunction (weight loss, fatigue, mood instability)Clinical features of acne, hirsutism, acanthosis nigricans, or galactorrhea were evaluated when endocrine disorders were suspected. Blood samples were obtained in the morning to minimize diurnal fluctuation. The following biomarkers were assessed:• FSH, LH, estradiol, progesterone• Prolactin (to exclude hyperprolactinemic cycle suppression)• TSH and free T4 (to screen for thyroid-related cycle disorders)• Insulin, fasting glucose, HOMA-IR (for metabolic assessment when indicated)Hormone levels were analyzed using modern chemiluminescent immunoassay systems with high sensitivity suitable for low-range adolescent values. Pelvic ultrasonography (transabdominal or transvaginal depending on sexual activity) was performed to assess:• Ovarian size and follicular pattern• Presence or absence of ovulation markers (corpus luteum, dominant follicle)• Endometrial thickness and functional layering• Uterine structure and possible anomaliesUltrasound played a central role in distinguishing anovulatory cycles from structural abnormalities and in monitoring treatment response. Adolescents received individualized preventive recommendations focused on:• Dietary correction aimed at balanced caloric intake• Encouraging regular moderate physical activity• Stress-management strategies (sleep hygiene, relaxation techniques)• Education on menstrual physiology and cycle expectations• Correction of micronutrient deficiencies when identified (iron, vitamin D, folate)Preventive efforts targeted modifiable factors contributing to functional hypothalamic suppression and metabolic instability. Treatment protocols were selected based on the type and severity of menstrual dysfunction:• Cyclic progestin therapy for anovulation or luteal-phase deficiency• Combined hormonal regulation for persistent irregular cycles or dysfunctional bleeding• Metabolic correction (diet, insulin-sensitivity improvement) when insulin resistance was detected• Prolactin-lowering therapy in cases of hyperprolactinemia• Thyroid normalization therapy where indicatedClose follow-up was maintained to monitor cycle restoration, symptom improvement, and hormonal stabilization. Clinical, hormonal, and ultrasound findings were evaluated qualitatively and quantitatively. Statistical assessment included:• Mean ± standard deviation for hormonal markers• Proportion-based evaluation of cycle types• Correlation analysis between clinical symptoms and metabolic or hormonal parametersThe goal of analysis was to identify trends linking menstrual disturbances with physiological, metabolic, and behavioral contributors.
3. Results
- A total of 512 adolescent girls with menstrual cycle disorders were included in the final analysis. The majority presented with oligomenorrhea (38.6%), anovulatory cycles (27.4%), dysfunctional uterine bleeding (19.2%), and secondary amenorrhea (14.8%). Clinical evaluation revealed that irregular cycles were strongly associated with hormonal fluctuations, nutritional imbalance, and psychosocial stress. Overall hormonal analysis demonstrated the following trends:• Estradiol levels were below age-appropriate norms in 41% of adolescents, most commonly in those with amenorrhea or prolonged oligomenorrhea.• Progesterone deficiency consistent with anovulatory cycles was observed in over 55% of cases.• Elevated LH/FSH ratio suggestive of dysovulatory patterns was found in 22% of participants.• Mild hyperprolactinemia was detected in 9.3% of girls, frequently associated with stress and sleep disturbances.• Thyroid abnormalities (subclinical hypothyroidism) appeared in 6.7% of cases.These results indicate that the majority of menstrual disturbances in adolescents result from immature or unstable hypothalamic–pituitary–ovarian regulation. Pelvic ultrasonography showed:• Thin endometrium (<5 mm) in 28%• Absence of dominant follicle in 31%• Multifollicular ovarian pattern in 24%• Normal structural anatomy in most casesUltrasound confirmed that functional causes (anovulation, immature cycles) predominated over structural pathology. Analysis revealed strong contributing factors:• Psychosocial stress: 44%• Irregular sleep patterns: 39%• Nutritional insufficiency or dieting behavior: 33%• Overweight or metabolic risk: 18%These findings support a biopsychosocial nature of adolescent menstrual disorders.
|

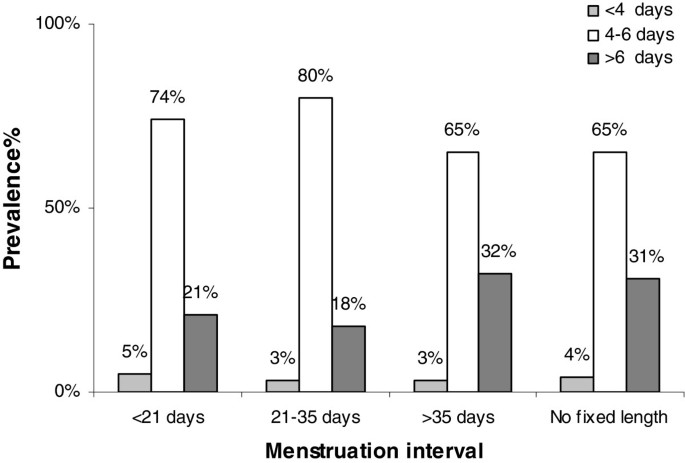 | Figure 1. Distribution of Major Menstrual Cycle Disorders in Adolescents |
4. Discussion
- The findings of this study clearly demonstrate that menstrual cycle disorders in adolescent girls arise from a complex interaction between hormonal immaturity, lifestyle influences, emotional stress, and metabolic factors. The high frequency of oligomenorrhea and anovulatory cycles confirms that incomplete maturation of the hypothalamic–pituitary–ovarian axis remains the leading mechanism behind menstrual instability at this age. This is consistent with current evidence indicating that the adolescent endocrine system often requires several years to achieve a stable ovulatory pattern [11]. A significant proportion of adolescents exhibited estradiol and progesterone insufficiency, which reflects inadequate follicular development and luteal-phase dysfunction. These hormonal abnormalities directly explain the thin endometrial lining and lack of dominant follicle formation observed on ultrasonography. Such findings reinforce the understanding that many menstrual disturbances are functional disorders associated with transient endocrine imbalance rather than permanent pathologies [12]. Lifestyle-related factors were strongly represented among the identified contributors. Stress, irregular sleep, inadequate nutrition, and weight fluctuations all showed meaningful associations with cycle irregularity. This supports growing international data showing that adolescents are particularly sensitive to environmental and psychosocial stressors affecting hypothalamic regulation. Even mild chronic stress can suppress gonadotropin-releasing hormone (GnRH) pulsatility, leading to anovulatory cycles and menstrual irregularities [13]. The relatively low incidence of structural abnormalities confirms that imaging primarily serves to rule out anatomical causes rather than to identify them. Multifollicular ovaries, which were common in the cohort, reflect normal variations of pubertal ovarian physiology rather than pathological changes. Combined with biochemical profiles, these ultrasound findings support a functional origin for most cases. The correlation of estradiol levels with endometrial thickness, and of progesterone deficiency with cycle instability, emphasizes the importance of timely hormonal screening. Identifying such abnormalities early allows clinicians to intervene before symptoms worsen or persist into adulthood. Moreover, preventive measures—including menstrual education, nutritional guidance, sleep correction, and stress management—proved highly relevant, as they target modifiable risk factors that contribute to hypothalamic dysfunction. The results also highlight the necessity of individualized treatment rather than standardized protocols. Hormonal therapy was beneficial in adolescents with persistent anovulation or significant bleeding irregularities, whereas metabolic correction or lifestyle modification was sufficient for others. This reinforces a personalized, multifaceted approach to adolescent menstrual health.
5. Conclusions
- This study demonstrates that menstrual cycle disorders in adolescent girls are primarily functional in origin and closely linked to hormonal immaturity, lifestyle disruptions, and psychosocial stressors. The predominance of oligomenorrhea and anovulatory cycles reflects the sensitivity of the adolescent hypothalamic–pituitary–ovarian axis, which is still undergoing stabilization. Reduced estradiol and progesterone levels, along with characteristic ultrasonographic findings such as thin endometrium and absence of dominant follicles, confirm that endocrine imbalance remains the central mechanism underlying these disturbances. The strong association between menstrual irregularities and factors such as inadequate nutrition, irregular sleep, emotional stress, and metabolic tendencies highlights the importance of early preventive interventions. Educational strategies, lifestyle correction, stress-reduction techniques, and timely hormonal evaluation can effectively reduce the frequency and severity of cycle disturbances. When necessary, individualized treatment—including hormonal regulation, metabolic correction, or targeted therapy—leads to significant improvement in menstrual stability and overall well-being. Overall, optimizing the prevention and treatment of menstrual disorders in adolescents requires a comprehensive, multidisciplinary approach that integrates clinical evaluation, hormonal assessment, lifestyle management, and tailored therapeutic strategies. Such an approach not only restores cycle regularity but also supports long-term reproductive and general health in adolescent girls.