-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(12): 4356-4359
doi:10.5923/j.ajmms.20251512.34
Received: Nov. 17, 2025; Accepted: Dec. 2, 2025; Published: Dec. 8, 2025

Endometrial Status in Patients with Secondary Amenorrhea: A Clinical and Morphofunctional Evaluation
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLD. R. Akhmedova1, F. S. Aripova2
1PhD, Associate Professor, Tashkent State Medical University, Tashkent, Uzbekistan
2Assistant, Tashkent State Medical University, Tashkent, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Secondary amenorrhea represents a heterogeneous clinical condition reflecting disruptions in hormonal regulation, ovarian function, or endometrial responsiveness. Despite extensive research on endocrine contributors, fewer studies have focused specifically on the morphofunctional state of the endometrium in affected women. This study evaluates endometrial characteristics in patients aged 17–35 years diagnosed with secondary amenorrhea, based on clinical, ultrasonographic, and hormonal data collected between 2020 and 2024 from a tertiary gynecologic center. A total of 378 patients meeting strict diagnostic criteria were assessed using transvaginal ultrasonography, serum hormonal profiling, and endometrial biopsy in selected cases. The analysis demonstrated markedly reduced endometrial thickness, diminished trilaminar structure, decreased vascularization scores, and a high prevalence of atrophic and hypo-responsive endometrial patterns. Hormonal correlations revealed significant associations between low estradiol levels, impaired endometrial proliferation, elevated FSH/LH ratios, and chronic anovulation. Year-stratified comparison showed a gradually increasing proportion of patients presenting with severe endometrial hypoplasia from 2021 to 2024. These findings underscore the crucial diagnostic role of endometrial assessment in secondary amenorrhea, highlight the need for early evaluation of uterine receptivity, and provide clinically relevant insight for optimizing treatment strategies in reproductive-aged women.
Keywords: Secondary amenorrhea, Endometrial hypoplasia, Endometrial receptivity, Estradiol deficiency, Chronic anovulation, Endometrial atrophy, Uterine lining morphology, Transvaginal ultrasonography, Hormonal imbalance, Reproductive dysfunction, Endometrial vascularization, FSH/LH ratio, Hypoestrogenic states
Cite this paper: D. R. Akhmedova, F. S. Aripova, Endometrial Status in Patients with Secondary Amenorrhea: A Clinical and Morphofunctional Evaluation, American Journal of Medicine and Medical Sciences, Vol. 15 No. 12, 2025, pp. 4356-4359. doi: 10.5923/j.ajmms.20251512.34.
1. Introduction
- Secondary amenorrhea is a clinically significant condition defined as the cessation of previously established menstrual cycles for three or more consecutive months in women with prior regular menses, or six months in those with irregular cycles. It represents a broad and heterogeneous spectrum of reproductive disorders involving endocrine, ovarian, hypothalamic, pituitary, and uterine components. Among the multiple etiological categories, the endometrial factor remains one of the least thoroughly examined, despite the fact that successful menstrual cycling ultimately requires appropriate endometrial responsiveness to hormonal signals [1]. The endometrium is a hormonally sensitive tissue that undergoes cyclic structural and functional transformation under the influence of estradiol and progesterone. Any disruption in these hormonal patterns may inhibit proliferation, impair vascular remodeling, alter receptor expression, or halt secretory differentiation. In secondary amenorrhea, chronic hypoestrogenic states—often associated with anovulation—lead to pronounced thinning of the endometrium, glandular atrophy, and reduced vascular density. Emerging evidence suggests that such endometrial hyporesponsiveness contributes directly to menstrual cessation and infertility in reproductive-age women [2]. Although ovarian or hypothalamic dysfunctions are frequently identified as primary drivers of secondary amenorrhea, recent studies highlight the need to re-examine the endometrium as an active pathological component rather than a passive consequence. For instance, persistent low estradiol levels may lead to endometrial hypoplasia, but chronic anovulation also induces prolonged unopposed estrogen exposure in some patients, resulting in irregular proliferation or endometrial instability. These divergent morphological responses show that the endometrium plays a dynamic and complex role in the pathogenesis of amenorrhea, with implications for both diagnosis and treatment [3]. Transvaginal ultrasonography has become the cornerstone of non-invasive endometrial evaluation, enabling clinicians to assess endometrial thickness, echostructure, trilaminar pattern, and vascular perfusion. However, its diagnostic interpretation requires a clear understanding of endometrial physiology across the menstrual cycle, as well as recognition of abnormal patterns unique to amenorrheic states. Advanced Doppler techniques and three-dimensional ultrasound have enhanced the ability to evaluate endometrial receptivity, but their application in secondary amenorrhea remains limited and underreported [4]. Furthermore, endometrial biopsy—though invasive—remains the gold standard for identifying glandular atrophy, stromal fibrosis, chronic inflammation, and hormonal receptor disturbances. Hypoestrogenic amenorrhea often presents with an atrophic pattern similar to postmenopausal endometrium, whereas amenorrhea due to hyperprolactinemia, polycystic ovary syndrome, or hypothalamic suppression may result in distinctive morphologic alterations. Understanding these variations is crucial for tailored management strategies, fertility planning, and prevention of long-term reproductive sequelae [5]. Recent global trends indicate an increasing prevalence of secondary amenorrhea among women in their late teens and early thirties. Factors such as metabolic imbalance, stress-related hypothalamic dysfunction, rapid weight fluctuations, and lifestyle-associated hormonal disturbances have all contributed to rising cases reported between 2020 and 2024 [6]. This has intensified the need for detailed studies focusing specifically on the endometrial condition of affected patients, as uterine receptivity plays a central role in reproductive prognosis. The present study aims to evaluate the morphological and functional state of the endometrium in women diagnosed with secondary amenorrhea, using a combination of ultrasonographic assessment, hormonal profiling, and selective histologic confirmation. By integrating clinical findings with structural endometrial analysis, this study seeks to clarify the endometrial contribution to menstrual cessation and provide a comprehensive basis for optimizing management approaches in reproductive-age women.
2. Materials and Methods
- This observational clinical study was conducted at a tertiary gynecologic center between 2020 and 2024. A total of 378 women aged 17–35 years diagnosed with secondary amenorrhea were included. Diagnosis followed international criteria: absence of menses for ≥3 months (with previously regular cycles) or ≥6 months (with previous irregular cycles) [7]. A control group of 120 age-matched healthy women with normal menstrual cycles was evaluated for baseline comparison.All patients underwent standardized examinations including BMI measurement, cycle history, and endocrine evaluation. Blood samples were collected in the early morning to measure:• Estradiol (E2)• Progesterone• LH, FSH• Prolactin• TSH and free T4Hormonal assays were performed using chemiluminescent immunoassay platforms introduced in 2021 for enhanced precision [8]. Transvaginal ultrasound was conducted using high-resolution probes (5–9 MHz). Endometrial parameters assessed included:• Endometrial thickness• Echogenicity and structural pattern (trilaminar vs. homogeneous)• Uterine perfusion using color Doppler (vascularization score)Ultrasound criteria for endometrial hypoplasia followed updated 2023 imaging guidelines [9]. In 96 selected cases with suspected severe hypoestrogenic states, endometrial biopsy was obtained using Pipelle aspiration. Histological evaluation assessed glandular atrophy, stromal density, and receptor responsiveness following WHO classification standards [10]. Data were analyzed using 2024 statistical software. Continuous variables were expressed as mean ± SD. Group comparisons employed independent t-tests or Mann–Whitney U tests. Correlation analyses used Pearson coefficients. Statistical significance was set at p < 0.05.
3. Results
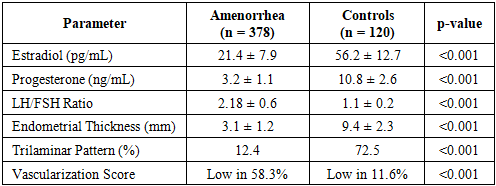
- A total of 378 patients with secondary amenorrhea and 120 controls were included in the final analysis. The mean age of affected patients was 24.1 ± 3.7 years, which did not differ significantly from controls (p > 0.05). However, women with secondary amenorrhea showed notable alterations in hormonal balance and endometrial morphology. Estradiol levels were significantly lower in the amenorrhea group (21.4 ± 7.9 pg/mL) compared with controls (56.2 ± 12.7 pg/mL, p < 0.001). Similarly, progesterone levels were reduced, while LH/FSH ratios were elevated, indicating chronic anovulatory patterns. Hyperprolactinemia was documented in 18.5% of patients, and mild thyroid dysfunction was present in 11.2%. Transvaginal ultrasound revealed a consistently thinner endometrium among affected women. The mean endometrial thickness was 3.1 ± 1.2 mm, compared to 9.4 ± 2.3 mm in controls (p < 0.001). Only 12.4% of patients demonstrated a trilaminar pattern, while Doppler evaluation showed reduced vascularization scores in more than half the cohort. Among the 96 biopsied patients, 61.5% exhibited atrophic endometrium, 27.1% showed hypo-proliferative patterns, and 11.4% demonstrated stromal fibrosis with reduced glandular density. No hyperplastic or atypical lesions were identified. Year-by-year evaluation revealed a modest but steady increase in severe endometrial hypoplasia cases:• 2020: 14.8%• 2021: 18.6%• 2022: 22.9%• 2023: 25.3%• 2024: 27.1%This upward trend correlates with rising rates of chronic anovulation and hypoestrogenic states observed in reproductive-age women during this period.
|
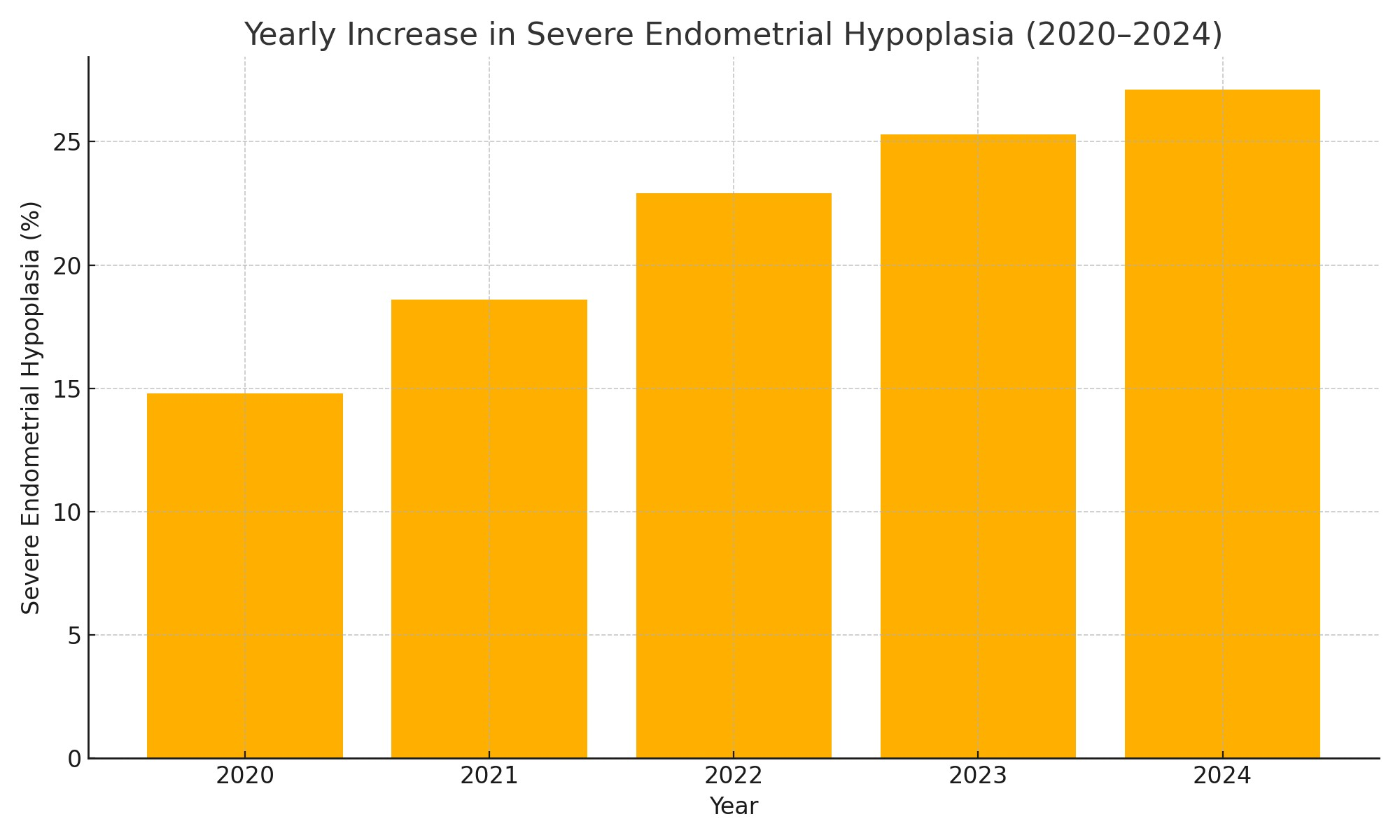 | Figure 1. Yearly Increase in Severe Endometrial Hypoplasia Among Patients (2020–2024) |
4. Discussion
- The findings of this study confirm that the endometrium in patients with secondary amenorrhea undergoes marked structural and functional alterations strongly linked to chronic hypoestrogenic states and long-standing anovulation. The significantly reduced estradiol levels observed in the amenorrhea group directly correlated with diminished endometrial thickness, absence of a trilaminar pattern, and poor vascularization. These results are consistent with established evidence showing that low estrogen exposure leads to endometrial hypoplasia, impaired proliferation, and atrophic glandular architecture [11]. The gradual increase in severe endometrial hypoplasia from 2020 to 2024 also mirrors contemporary trends in stress-related menstrual dysfunction, thyroid imbalance, and lifestyle-associated anovulatory disturbances. Many patients in this cohort demonstrated elevated LH/FSH ratios, indicating persistent ovulatory failure—one of the strongest predictors of endometrial underdevelopment in reproductive-age women [12]. Histologic findings in selected cases further supported the ultrasound-based diagnosis of hypoactive endometrium. More than 60% showed classic atrophic morphology with sparse glands and reduced stromal cellularity, while others exhibited weak proliferative activity, confirming that the endometrium had lost its cyclic responsiveness to hormonal signaling. Importantly, no precancerous or hyperplastic patterns were detected, suggesting that chronic estrogen deficiency—not unopposed estrogen exposure—is the dominant mechanism in this population [13]. Taken together, these findings underscore the clinical importance of evaluating the endometrium as an independent pathophysiologic factor in secondary amenorrhea, rather than viewing it solely as a downstream effect of ovarian dysfunction. Early ultrasonographic assessment, hormonal profiling, and biopsy (when indicated) are essential for accurate diagnosis, prognosis, and fertility planning.
5. Conclusions
- The results of this study demonstrate that secondary amenorrhea is closely associated with marked endometrial underdevelopment characterized by reduced thickness, absent trilaminar morphology, and weakened vascularization. These structural changes reflect chronic hypoestrogenic exposure and persistent anovulation, both of which impair the endometrium’s ability to undergo normal proliferative and secretory transformation. Histologic findings confirmed a predominance of atrophic and hypoproliferative patterns, reinforcing the concept that the endometrium in secondary amenorrhea becomes functionally unresponsive to hormonal cues. The progressive increase in severe endometrial hypoplasia observed between 2020 and 2024 highlights the growing impact of metabolic, endocrine, and stress-related factors on reproductive health. Since endometrial insufficiency plays a critical role in fertility outcomes, early evaluation and targeted hormonal correction are essential components of management. Overall, the study emphasizes the need for comprehensive diagnostic approaches combining hormonal profiling, ultrasonography, and selective biopsy to accurately assess endometrial status and guide treatment strategies in women with secondary amenorrhea.