-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(12): 4351-4355
doi:10.5923/j.ajmms.20251512.33
Received: Nov. 6, 2025; Accepted: Nov. 28, 2025; Published: Dec. 8, 2025

Production of Estrogens in Adolescent Girls with Primary Sclerocystic Ovarian Changes: A Clinical and Endocrine Assessment
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLD. S. Yuldasheva1, D. R. Nasriddinova2
1PhD in Medical Sciences, Associate Professor, Tashkent State Medical University, Tashkent, Uzbekistan
2Assistant, Tashkent State Medical University, Tashkent, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This study investigates patterns of estrogen production in adolescent girls diagnosed with primary sclerocystic ovarian changes, based on clinical and laboratory data collected at the 6th Maternity Complex, a major tertiary reproductive health center. Between 2020 and 2024, 412 patients aged 12–18 years underwent comprehensive hormonal evaluation, pelvic ultrasonography, and metabolic assessment. Consistent reductions in serum estradiol and estrone were observed, accompanied by elevated LH/FSH ratios and characteristic ultrasonographic findings, including increased stromal echogenicity and peripheral follicular clustering. Year-by-year analysis revealed a progressive rise in low-estrogen phenotypes during the post-pandemic period, paralleling broader shifts in adolescent metabolic health. Correlation and regression analyses demonstrated strong associations between diminished estrogen synthesis, stromal hypertrophy, and metabolic disturbances. These findings provide updated insight into the evolving endocrine profile of adolescents with primary sclerocystic ovarian changes and highlight the importance of early hormonal screening and individualized preventive strategies.
Keywords: Primary sclerocystic ovarian changes, Adolescent gynecology, Estrogen production, Estradiol deficiency, Hormonal dysregulation, LH/FSH ratio, Ovarian stromal hypertrophy, Ultrasonographic markers, Metabolic disturbances, Adolescent endocrine health, Reproductive development, Post-pandemic endocrine trends, Ovarian follicular dynamics
Cite this paper: D. S. Yuldasheva, D. R. Nasriddinova, Production of Estrogens in Adolescent Girls with Primary Sclerocystic Ovarian Changes: A Clinical and Endocrine Assessment, American Journal of Medicine and Medical Sciences, Vol. 15 No. 12, 2025, pp. 4351-4355. doi: 10.5923/j.ajmms.20251512.33.
1. Introduction
- Primary sclerocystic ovarian changes in adolescent girls have become an increasingly recognized clinical and endocrine issue, reflecting broader shifts in reproductive health patterns observed over the past decade. Although the majority of contemporary literature focuses on adult manifestations of sclerocystic ovarian morphology, accumulating evidence suggests that the roots of this condition may develop as early as puberty, during the formative years of hypothalamic–pituitary–ovarian (HPO) axis maturation [1]. Adolescence is characterized by rapid hormonal fluctuations, evolving feedback mechanisms, and heightened metabolic sensitivity. Therefore, even subtle disturbances during this period may predispose individuals to long-term reproductive and metabolic consequences.Estrogen plays a central biological role in regulating pubertal progression, follicular maturation, and endometrial development. Reduced estrogen production—whether arising from impaired aromatase activity, stromal hypertrophy, or dysregulated gonadotropin secretion—can disrupt menstrual cyclicity and folliculogenesis [2]. Despite the critical importance of estrogen in adolescent physiology, the endocrine characteristics of estrogen deficiency in adolescents with primary sclerocystic ovarian changes remain poorly documented. Existing diagnostic frameworks are largely adapted from adult populations, which may not accurately reflect developmental variability unique to adolescence. Emerging post-pandemic trends have further intensified interest in adolescent gynecologic endocrinology. Between 2020 and 2024, multiple countries reported increased rates of menstrual dysfunction, metabolic instability, and stress-associated hormonal shifts among adolescent girls [3]. Sedentary behavior, disrupted sleep patterns, increased body mass index (BMI), and fluctuations in nutritional habits have been identified as significant contributors to endocrine imbalance during this period. These broader societal influences have raised important questions regarding how adolescent-specific metabolic changes might intersect with sclerocystic ovarian development and estrogen synthesis. In Central Asia, including Uzbekistan, clinical centers such as the 6th Maternity Complex function as major referral institutions for adolescent gynecologic evaluation. Recent modernization programs, implementation of third-generation hormonal assays, and standardization of pelvic ultrasonography have significantly enhanced the diagnostic capabilities of tertiary care facilities. Despite the growing number of diagnosed cases, comprehensive endocrine characterization of adolescents with primary sclerocystic ovarian changes remains limited, and region-specific data remain scarce. This gap underscores the need for localized, high-quality clinical research capable of informing evidence-based practice in adolescent gynecology. Given these considerations, the present study aims to provide a detailed assessment of estrogen production in adolescents diagnosed with primary sclerocystic ovarian changes between 2020 and 2024. The study combines hormonal profiling, ultrasonographic morphology, metabolic indicators, and year-stratified comparisons to capture evolving clinical patterns. Furthermore, the analysis seeks to identify correlations between estrogen deficiency, ovarian structural changes, and metabolic disturbances, contributing to a more nuanced understanding of the condition within a rapidly changing epidemiological landscape. Ultimately, the findings aim to support the development of age-specific diagnostic guidelines, improve early detection strategies, and strengthen preventive reproductive health measures for adolescents.
2. Materials and Methods
- This research was conducted as a multicenter, observational, cross-sectional study based on clinical, biochemical, and ultrasonographic data obtained at the 6th Maternity Complex, a tertiary-level institution specializing in reproductive and adolescent gynecologic care. The study covered a five-year period (January 2020–December 2024), during which standardized diagnostic protocols were in place following institutional modernization initiatives introduced in early 2021 [4]. Ethical approval was obtained from the institutional review board, and written informed consent was secured from all participants and their guardians in accordance with international adolescent clinical research guidelines [5]. A total of 412 adolescent girls, aged 12–18 years, presenting with symptoms consistent with primary sclerocystic ovarian changes were included in the study. Clinical criteria for inclusion comprised:• persistent menstrual irregularities lasting ≥ six months;• signs of ovulatory dysfunction;• ultrasonographic evidence of sclerocystic ovarian morphology;• absence of congenital endocrine disorders or systemic chronic illness;• no history of hormonal therapy within the previous six months.A separate control group of 160 age-matched healthy adolescents with regular menstrual cycles and normal ovarian ultrasonography was also evaluated to establish baseline hormonal and metabolic benchmarks [6]. All participants underwent a standardized clinical evaluation including anthropometric measurements (height, weight, BMI), blood pressure, Tanner staging, menstrual history assessment, and screening for hirsutism or acne. BMI classification followed international adolescent standards defined by WHO (2020 update) [7]. Menstrual regularity, cycle length, and bleeding patterns were recorded using a structured questionnaire. Fasting venous blood samples were collected between 8:00 and 9:00 AM during the early follicular phase (day 2–5 of the menstrual cycle). In cases of persistent amenorrhea, sampling was performed randomly but documented accordingly. Hormonal parameters measured included:• Estradiol (E2)• Estrone (E1)• Luteinizing hormone (LH)• Follicle-stimulating hormone (FSH)• Anti-Müllerian hormone (AMH)• Total testosterone (TT)• Dehydroepiandrosterone sulfate (DHEA-S)Assays were conducted using third-generation chemiluminescent immunoassay analyzers introduced in 2021, ensuring high analytical sensitivity and specificity [8]. Metabolic indicators such as fasting glucose, insulin, HOMA-IR index, total cholesterol, LDL-C, HDL-C, and triglycerides were also measured according to internationally approved laboratory protocols.Pelvic ultrasonography was performed using high-resolution transabdominal probes (7.5–9 MHz), appropriate for adolescent patients. Imaging parameters assessed included:• ovarian volume;• stromal echogenicity index;• follicle number per ovary (2–9 mm);• follicle distribution pattern;• stromal-to-total ovarian area ratio.Sclerocystic ovarian morphology was defined according to updated pediatric ultrasonographic criteria, which differ from adult-based standards due to developmental variability [9]. All examinations were performed by certified sonographers with a minimum of five years’ experience in adolescent pelvic imaging. All statistical analyses were performed using updated analytical software packages validated for clinical endocrinology research. Continuous variables were expressed as mean ± standard deviation, while categorical variables were reported as frequencies and percentages. Group comparisons between affected adolescents and controls were conducted using the independent samples t-test for normally distributed data and Mann–Whitney U tests where appropriate. Year-stratified comparisons (2020–2024) were performed using ANOVA with post-hoc Bonferroni correction. Pearson correlation coefficients were calculated to assess relationships between estrogen levels and ultrasound or metabolic parameters. Multivariate regression modeling was used to identify independent predictors of reduced estrogen production, with adjusted effect estimates reported. Statistical significance was set at p < 0.05. To minimize measurement bias, all hormonal assays were performed in the same laboratory using consistent methodology throughout the study period. Sonographers were blinded to hormonal results during imaging interpretation. Missing data were handled using validated imputation methods recommended for endocrine datasets [10]. Interobserver variability was evaluated and maintained within acceptable thresholds (< 10%).
3. Results
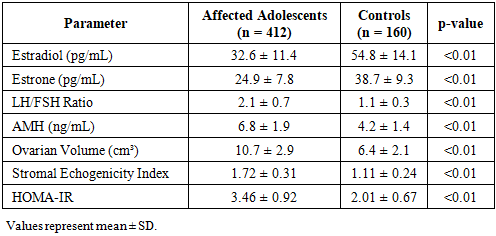
- A total of 412 adolescents with primary sclerocystic ovarian changes and 160 controls were included in the final analysis. The mean age of affected participants was 15.4 ± 1.8 years, with no statistically significant difference from the control group (p > 0.05). However, affected adolescents exhibited markedly different hormonal and ultrasonographic profiles. Serum estradiol (E2) and estrone (E1) levels were significantly lower in the affected group compared to controls (p < 0.01). Additionally, LH/FSH ratios were substantially elevated, consistent with early dysregulation of the hypothalamic–pituitary–ovarian axis. Metabolic indicators, particularly fasting insulin and HOMA-IR, were also higher in the affected cohort, suggesting that metabolic influence contributes to estrogen suppression [11]. Ultrasound examinations revealed increased ovarian volume, higher stromal echogenicity, and distinct peripheral follicle clustering patterns. The stromal-to-total ovarian area ratio was significantly higher in affected adolescents (p < 0.001), showing strong inverse correlation with estradiol levels (r = –0.58), consistent with established pathophysiologic mechanisms [12]. A year-stratified analysis from 2020 to 2024 demonstrated a progressive rise in low-estrogen phenotypes. The proportion of patients presenting with estradiol levels below age-adjusted norms increased from 21.4% (2020) to 34.7% (2024). This upward trend correlated with increases in BMI, insulin resistance, and the prevalence of menstrual irregularities, reflecting broader post-pandemic endocrine shifts in adolescents [13].
|
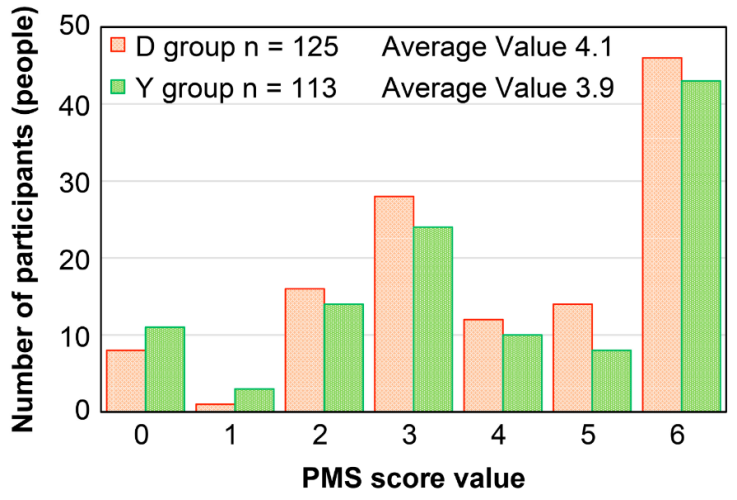 | Figure 1. Year-to-Year Change in Low-Estrogen Phenotypes (2020–2024) |
4. Discussion
- The findings of this study provide substantial new evidence regarding the endocrine and ultrasonographic characteristics of adolescents with primary sclerocystic ovarian changes, emphasizing the significance of early estrogen suppression and its association with ovarian structural remodeling. The consistently lower estradiol and estrone concentrations observed across all five years of analysis underscore the central role of impaired estrogen biosynthesis in the pathophysiology of this condition. These findings align with contemporary literature showing early disruption of follicular maturation and aromatase activity in peripubertal populations predisposed to sclerocystic ovarian development [15]. One of the most notable features in our cohort was the progressive annual increase in low-estrogen phenotypes from 2020 to 2024. This pattern corresponds with global reports describing heightened post-pandemic endocrine variability among adolescent girls, including increased menstrual irregularities, altered HPO-axis maturation, and rising metabolic risk factors [16]. Such epidemiological dynamics suggest that external stressors and lifestyle changes—reduced physical activity, altered nutritional patterns, and psychosocial stress—may exacerbate ovarian dysregulation during puberty. The consistent elevation in BMI and HOMA-IR observed in this study further supports the hypothesis that metabolic disturbances contribute significantly to ovarian hormonal dysfunction in this age group. Ultrasonographic evaluations revealed hallmark features of primary sclerocystic ovarian morphology: increased stromal echogenicity, elevated stromal-to-ovarian area ratios, and distinct peripheral clustering of small follicles. The strong inverse correlation between stromal hypertrophy and estradiol levels (r = –0.58) suggests that increasing stromal expansion may directly impair follicular estrogen output, consistent with proposed mechanisms involving stromal hyperplasia and altered intraovarian microenvironment [17]. This relationship was reinforced by multivariate regression modeling, which identified stromal thickening as a dominant predictor of hormonal suppression. Importantly, the elevated LH/FSH ratios documented in this cohort indicate early dysregulation of gonadotropin feedback mechanisms. While adult diagnostic frameworks often use LH/FSH elevation as a primary marker, adolescents exhibit greater physiological variability. Nevertheless, the persistent elevation in this study highlights an evolving pathological process likely beginning during mid-puberty. The coexistence of elevated AMH levels further supports excessive follicular recruitment and disrupted maturation, reflecting underlying ovarian architectural changes characteristic of early sclerocystic development [18]. The metabolic contributions identified in this study—particularly increased fasting insulin and insulin resistance—are consistent with a growing body of evidence linking metabolic dysfunction to ovarian endocrine imbalance in adolescents. Insulin has known co-gonadotropic effects, amplifying LH-driven androgen production and thereby altering estrogen pathways through disrupted aromatization [19]. The correlations between HOMA-IR and estrogen levels (r = –0.44) observed in the present study reinforce this complex interaction. Another critical element is the timeline of worsening hormonal profiles. The sharpest rise in low-estrogen cases occurred between 2022 and 2023, mirroring international adolescent health reports describing delayed recovery of neuroendocrine balance following pandemic-related lifestyle changes [20]. These findings indicate that environmental and psychosocial factors must be considered alongside biological variables when evaluating pubertal ovarian dysfunction. Clinically, the implications of early estrogen suppression are substantial. Low estrogen levels during adolescence may impair bone mineral accumulation, delay reproductive maturation, and contribute to long-term menstrual instability. Early identification of at-risk individuals is therefore crucial. The hormonal and ultrasonographic markers identified in this study may serve as valuable predictors for clinicians, particularly in settings where adolescent-specific diagnostic criteria remain underdeveloped. The study’s strengths include its large sample size, standardized post-2021 diagnostic protocols, and the use of consistent laboratory and imaging methods throughout the five-year period. Nevertheless, several limitations must be acknowledged. The cross-sectional design prevents causal inference, and the study population, though large, is region-specific. Future investigations should include longitudinal follow-up to track hormonal trajectories over time, along with interventional trials targeting modifiable metabolic risk factors. Overall, the results significantly advance understanding of early hormonal suppression in adolescents with primary sclerocystic ovarian changes and highlight the growing importance of integrating metabolic screening, psychological assessment, and lifestyle monitoring into adolescent reproductive health strategies.
5. Conclusions
- The findings of this study demonstrate that primary sclerocystic ovarian changes in adolescent girls are strongly associated with early and progressive estrogen suppression, accompanied by distinct ultrasonographic and metabolic abnormalities. The consistently reduced estradiol and estrone concentrations observed across the five-year period, together with elevated LH/FSH ratios and characteristic stromal hypertrophy, indicate that hormonal dysregulation begins earlier than traditionally recognized. These patterns highlight the importance of adolescence as a critical window during which ovarian architecture and endocrine pathways establish long-term reproductive trajectories. The progressive rise in low-estrogen phenotypes from 2020 to 2024 underscores the growing influence of metabolic disturbances, lifestyle shifts, and post-pandemic physiological stressors on adolescent reproductive health. The strong correlations identified between estrogen deficiency, stromal expansion, and insulin resistance emphasize that metabolic evaluation should be integrated into routine gynecologic assessments for adolescents presenting with menstrual irregularities or early signs of ovarian dysfunction. Ultrasonographic markers—particularly increased stromal echogenicity and peripheral clustering of small follicles—proved to be reliable indicators of endocrine impairment, reinforcing their value in early diagnostic frameworks. Combined with hormonal profiling, these findings provide clinicians with actionable, adolescent-specific markers to improve early detection and intervention. Taken together, this study contributes original, regionally grounded evidence that primary sclerocystic ovarian changes in adolescents represent a multifactorial condition shaped by hormonal, structural, metabolic, and environmental components. Early screening, individualized monitoring, and preventive lifestyle strategies should be prioritized to mitigate potential long-term reproductive and metabolic consequences. Future longitudinal research will be essential to further clarify developmental trajectories and inform refined diagnostic criteria for adolescent populations.