-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(12): 4348-4350
doi:10.5923/j.ajmms.20251512.32
Received: Oct. 11, 2025; Accepted: Nov. 8, 2025; Published: Dec. 8, 2025

Features of Gynecological and Somatic History in Pregnant Women with Preeclampsia
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLNavruzova R. S., Khamidova Z. B.
Tashkent State Medical University, Tashkent, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Preeclampsia is a multifactorial syndrome characterized by hypertension and systemic endothelial dysfunction. It remains one of the leading causes of maternal and perinatal morbidity and mortality. Despite advances in modern perinatology, its pathogenesis is not fully understood, and prediction and prevention remain challenging. This study aims to assess the relationship between chronic inflammatory, infectious, and somatic diseases and the development of vascular and metabolic disorders underlying preeclampsia. By analyzing the gynecological and somatic history of pregnant women with varying severity of preeclampsia, we identify key risk factors and clarify its mechanisms, which are essential for early diagnosis, prevention, and improved pregnancy management strategies.
Keywords: Preeclampsia, Endothelial dysfunction, Risk factors, Inflammation, Pregnancy complications, Metabolic disorders
Cite this paper: Navruzova R. S., Khamidova Z. B., Features of Gynecological and Somatic History in Pregnant Women with Preeclampsia, American Journal of Medicine and Medical Sciences, Vol. 15 No. 12, 2025, pp. 4348-4350. doi: 10.5923/j.ajmms.20251512.32.
Article Outline
1. Introduction
- Preeclampsia is a multifactorial syndrome characterized by arterial hypertension and systemic endothelial dysfunction. Preeclampsia remains one of the leading causes of maternal and perinatal morbidity and mortality, ranking among the foremost complications of pregnancy [5,6,8]. Despite significant advances in modern perinatology, the pathogenesis of preeclampsia has not been fully elucidated, and the prediction and prevention of this complication remain challenging tasks [2,3,4].In recent years, particular attention has been paid to the role of chronic inflammatory, infectious, and somatic diseases in the development of vascular and metabolic disorders underlying preeclampsia [1,9,10]. The study of gynecological and somatic history in pregnant women with varying degrees of preeclampsia severity allows for the identification of the most significant risk factors and clarification of its developmental mechanisms, which is of great importance for early diagnosis, prevention, and the improvement of pregnancy management strategies [7].Aim of the StudyTo determine the features of gynecological and somatic history in pregnant women with severe preeclampsia compared with women without preeclampsia, in order to identify the factors contributing to the development and aggravation of this pregnancy complication.
2. Materials and Methods
- All pregnant women were examined at the Department of Obstetrics and Gynecology of the Tashkent Pediatric Medical Institute, at City Maternity Complex No. 6. An analysis of age characteristics among 113 women in the control and main groups revealed an average age of 28–29 years. The age of the examined women ranged from 20 to 41 years.
3. Analysis of Comorbidities
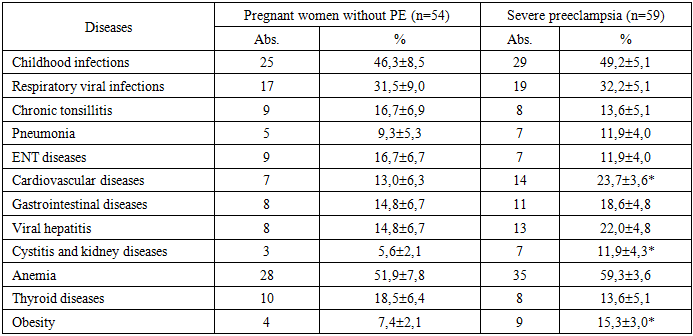
- According to the analysis of concomitant diseases (Table 1), anemia, childhood infections, and respiratory viral diseases were the most common conditions in both groups. Anemia was observed in 59.3 ± 3.6% of pregnant women with severe preeclampsia and in 51.9 ± 7.8% of women in the control group, indicating a high prevalence of this condition among pregnant women, although the difference between the groups was not statistically significant (p > 0.05). Childhood infections were reported in 49.2 ± 5.1% of women in the main group and 46.3 ± 8.5% in the control group, while respiratory viral diseases were noted in 32.2 ± 5.1% and 31.5 ± 9.0%, respectively. The incidence of chronic tonsillitis, pneumonia, and ENT disorders was comparable between the groups, with no statistically significant differences observed.
|
|

4. Results and Discussion
- The conducted analysis showed that pregnant women with severe preeclampsia are significantly more likely to present with inflammatory diseases of the reproductive system, such as colpitis, endocervicitis, chronic adnexitis, and a higher prevalence of infertility in medical history. These findings indicate a possible pathogenetic role of chronic infectious and inflammatory genital processes in the formation of vascular disorders and the development of preeclampsia. In addition, women with preeclampsia exhibit a tendency toward a higher prevalence of somatic diseases, particularly anemia, obesity, and urinary system pathology. The combination of infectious-inflammatory and metabolic disturbances may represent an unfavorable background that contributes to the development and exacerbation of preeclampsia.
5. Conclusions
- The obtained results emphasize the necessity of a comprehensive approach to the examination and management of pregnant women at risk, taking into account their gynecological and somatic history. Such an approach is essential for effective early prevention and timely management of pregnancy complications.