Karimov Komil Kamolovich
Bukhara State Medical Institute named after Abu Ali Ibn Sino, Bukhara, Uzbekistan
Correspondence to: Karimov Komil Kamolovich, Bukhara State Medical Institute named after Abu Ali Ibn Sino, Bukhara, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The first group included patients who received surgical removal of a portion of the nucleus pulposus within 72 hours from the time of radical ischemia (cauda syndromes) - 51 patients (43.2%), and the second group were included later than 72 hours from the time of the development of neurological manifestations of acute on - 67 (56.8%). Integrated clinical and neurological research in combination with paraclinics and instrumental methods such as the CT/MRI, allowed not only to clarify the functions of the roots of the cauda equina in precipitated a herniated intervertebral disc on lumbar level, but also to determine the correlation with the size of the hernia and direction of migration of the sequestrations fragment, as well as the degree of secondary stenosis of the vertebral canal.
Keywords:
Radiculopathy caused by herniated disc protrusion, Discogenic lumbosacral syndromes
Cite this paper: Karimov Komil Kamolovich, Discogenic Radiculoischemic Syndrome of the Lumbar Spine, American Journal of Medicine and Medical Sciences, Vol. 15 No. 12, 2025, pp. 4339-4344. doi: 10.5923/j.ajmms.20251512.30.
1. Introduction
Spinal pathology ranks 5th among the causes of hospitalization and 3rd among the causes of surgical treatment. The process of disability is also high: vertebrogenic lesions are observed in 80% of cases among people with disabilities with diseases of the peripheral nervous system. Radiculopathy caused by herniated disc protrusion, among other pathogenetic factors of this disease, occur in 80-86% of cases. Hernial protrusion affects the roots and radicular arteries in the epidural space, causing their compression and, as a result, spasm. More than 60% of people registered with a neurologist have been treating back and limb pain for a number of years, and reflex and compression discogenic syndromes of the lumbosacral level are diagnosed in up to 24% of cases [2,4,7,14]. Progress in the surgical treatment of herniated discs is closely related to accurate preoperative information about the nature of disc damage.In patients with discogenic lumbosacral radiculopathy, radicular and spinal ischemic disorders are noted in 32-38% of cases. Despite the widespread introduction of minimally invasive and high-tech methods of surgical treatment of intervertebral disc herniations, the number of operated patients with radiculomyeloischemic complications remains high and, according to various data, ranges from 1.5 to 20%. Existing surgical procedures for intervertebral disc herniations at the lumbosacral level, when ischemia of the root(s) and the corresponding area of the spinal cord occurs (which underlies the discogenic radiculomyeloischemic syndromes described in the literature), are primarily aimed at removing sequestered disc fragments that compress nerve roots and vascular formations, followed by revision of the intervertebral fissure and the cavity of the intervertebral disc, and, if necessary, resection of adjacent edges of the arches for decompression of the nerve root [1,3,8,9,20]. Ischemic complications develop, as a rule, acutely, usually during an exacerbation of radicular pain, at the height of the so-called hyperalgic coat. Neurological symptoms indicate a lesion in the anterior arterial basin. In most patients, surgery reveals an arterial vessel compressed with a herniated disc root. Some patients have a hypertrophied vein accompanying a compressed root [4,11,14]. Taking into account the anatomical structure of the root vessels and their surface location, venous stasis with impaired microcirculation of the ponytail occurs already with local compression of 10 mmHg, while the peripheral nerve can withstand pressure up to 200 mmHg. Clinically, radiculoischemia is divided into transient disorders of the radicular blood supply, acute blood supply disorders with blockage of conduction along the root and chronic violation of blood supply – compression-ischemic radiculopathy. The identification of variants of radiculoishemia is conditional – they represent links in a complex pathogenetic process - but it is important from a clinical point of view, since their timely diagnosis and correct interpretation largely determine treatment tactics and prognosis [7,11,18].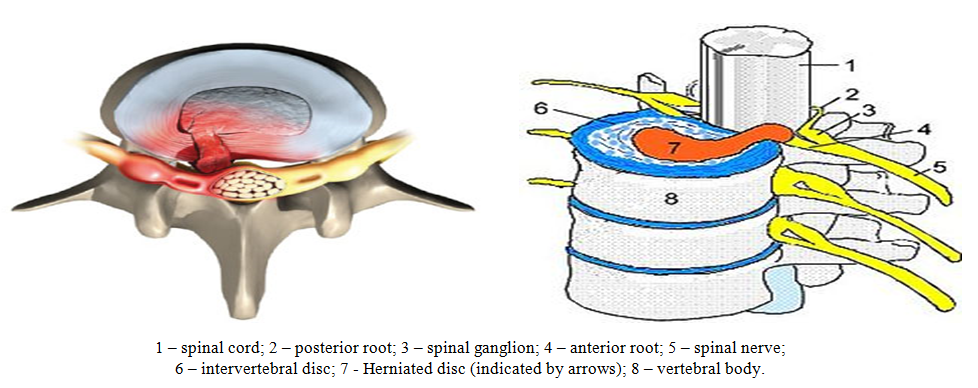 | Figure 1. General scheme of the spinal-motor segment |
Transient radiculoischemia can overlap with the clinic of reflex pain syndromes, when an objective examination has not yet revealed symptoms of prolapse in the innervation zone of the root. An acute circulatory disorder with a complete violation of root conduction – a kind of radicular infarction as a result of occlusion of the radicular artery – is well known in the clinic by the example of the so-called paralyzing sciatica. Chronic radiculoishemia leads to root fibrosis, demyelination and degeneration of nerve fibers. These changes are the result of dynamic and permanent venous, arterial, and microcirculatory disorders in people with spinal diseases that lead to stenosis of the radicular or spinal canals. Local ischemia of discogenic origin is an important link in the formation of acute radiculoischemia of the roots of the ponytail (Cauda syndrome). Dyscirculatory phenomena are manifested in the area of the affected spinal motor segments (VDS) and in the associated segments by a decrease in local blood flow in the epidural venous plexus system, which leads to the development of venous stasis and local epiduritis [17]. Ponytail syndrome (cauda equina syndrome) is a rare and serious condition that is considered an urgent condition and requires urgent medical attention. Cauda syndrome includes compression and ischemia of the ponytail, bundles of spinal nerve roots that descend from the epiconus of the spinal cord and include all spinal nerve roots below the level of the first lumbar vertebra (sacral and coccygeal nerves). This compression leads to dull pain in the lower back and buttocks, numbness of the anogynetal zone, impaired function of the bladder, rectum and external genitalia. Pressure on the nerves leads to the development of lesions in the nervous system, causing weakness of the bladder (neurogenic bladder) and loss of intestinal control due to weakness of the rectal sphincter. Men develop erectile dysfunction [6,7]. According to the literature in the USA, horsetail syndrome as a result of a herniated lumbar disc is registered annually from 1% to 15% of cases per 100,000 population. A herniated disc in the lumbar region is the cause of ponytail syndrome in 1-15% of cases. In 90% of cases, herniated discs occur at the level of 4-5 lumbar vertebrae and the 5th lumbar and 1st sacral vertebrae. In 70% of cases of herniated discs, which leads to ponytail syndrome, occur in people with chronic back pain, and in 30% of cases, ponytail syndrome may be the first manifestation of a herniated disc. Herniated disc, which leads to ponytail syndrome, occurs most often in men aged 30-40 years. In most cases of ponytail syndrome, which is caused by a herniated disc, large parts of the disc substance are affected, which completely separate from the normal disc and compress the nerve roots of the ponytail [7, 17]. Surgery is the method of choice in the treatment of this condition. In most cases of emergency decompression surgery, it relieves pressure on the nerves and prevents nerve damage. The timing of surgical decompression is controversial, but most doctors recommend surgery within 48 hours after the onset of cauda syndrome. The loss of time in patients with lumbar discogenic radiculomyeloischemia, and their late treatment for adequate surgical care, leads to the occurrence of severe and persistent neurological disorders (paresis of varying severity, paralysis, pelvic organ dysfunction, sensitivity disorders in the lower extremities, in the urogenital zone, etc.), poorly amenable to rehabilitation therapy and rehabilitation [10,12,13,15,16,19]. The aim of the work was to determine the correlation between acute discogenic radiculoishemia at the lumbar level and the size and direction of migration of the hernia sequester and the prescription of the development of acute radiculoishemic syndrome.
2. Material and Methods
The study was conducted on the basis of the Department of Emergency Neurosurgery of the Russian National Research Center for the period 2022-2023. We treated 118 patients with prolapsed monosegmental herniated discs (IVD) at the lumbar level with the development of acute radiculoischemic syndrome (Cauda syndrome), 46 of them men (38.98%), 72 women (61.02%), aged from 20 to 54 years (average age – 31.0±9.7 years). The patients were divided into 2 groups: 1st - 51 (43.2%) patients hospitalized with radiculoischemia on the background of a herniated IVD and frolicking for up to 72 hours; The 2nd group consisted of 67 (56.8%) patients who were hospitalized later than 72 hours after the onset of radiculoishemia. All patients underwent a standard neurological and vertebroneurological examination. Of the additional methods of examination, the following were used: classical radiography of the lumbosacral spine, computed tomography of the lumbar spine (MSCT) and/or magnetic resonance imaging (MRI). Taking into account the indications and contraindications, after analyzing the results of standard research methods, all patients underwent emergency surgical treatment.Table 1. Distribution of Patients
 |
| |
|
The structures of the affected spinal-motor segment (SPS) and local blood flow were studied in all patients according to the method of A.Y. Kinzersky [5]. Ultrasound examination of the lumbar spine was performed by anterior and posterolateral approaches using an energy Doppler. A multi-frequency convexic sensor (2.0-6.0 MHz) with a base frequency of 3.5 MHz was used. Anterior access was performed in the patient's supine position with legs bent at the knee joints. During the posterolateral scan, the patient sat on the couch with his back to the researcher, leaning forward as much as possible. The control was the ultrasound examination of the spine in 30 healthy individuals. A comprehensive clinical and diagnostic study made it possible to clarify the dysfunction of the roots of the ponytail with a prolapsed hernia of the IVD at the lumbar level and to determine the correlation between the prescription of the development of radiculoischemic syndrome with the size of the hernia and the direction of migration of the sequestered fragment. Pain syndrome of varying severity occurring in the lumbar spine and lower extremity (or two) during compression of the spinal root by herniated discs was observed in all patients. Special attention was paid to the presence of paresis or paralysis of the limb and NFT, as the most reliable symptoms of significant compression of the spinal root(s) or its vessel. When distributing patients, we followed a correlation between the age of development of radiculoischemic syndrome and the size, location and direction of sequestration of hernial protrusion. Neurological deficit developed acutely in 94 (79.7%) patients (within a few minutes or hours), while the remaining 14 (20.3%) patients experienced prolonged, sometimes unnoticeable, weakness of muscle groups (usually with mild paresis of the foot or paresis of the toes) upon admission to a neurosurgical hospital. Lower paraparesis was detected in 73 (61.9%) patients. Pelvic organ dysfunction (NFT) was observed in 102 (86.4%) patients. The assessment was based on impaired urination as the most sensitive and reliable symptom of NFTO. Urinary retention was determined in cases where the patient could not urinate without a catheter. Straining urination was diagnosed when it was necessary for the anterior abdominal wall to actively participate in the act of urination and for a long period of "waiting" before urination. The increase was recorded at a frequency of more than 6-7 acts per day. All patients underwent an assessment of the location of the prolapsed (sequestration) fragment of the IVD hernia along the diameter of the spinal canal (median, paramedian, posterolateral or foraminal), the degree of hernia prolapse (elastic protrusion, sequestered prolapse). We noted the following types of IVD hernias: median in 57 (48.3%), paramedial in 42 (35.6%), and lateral in 19 (16.1%) patients. Sensitivity disorders in dermatomes corresponding to compressed roots were observed in all patients. A complete absence of the Achilles reflex was noted in 89 (75.4%), a decrease in 29 (24.6%).Table 2. Variants of Intervertebral Disc Herniations
 |
| |
|
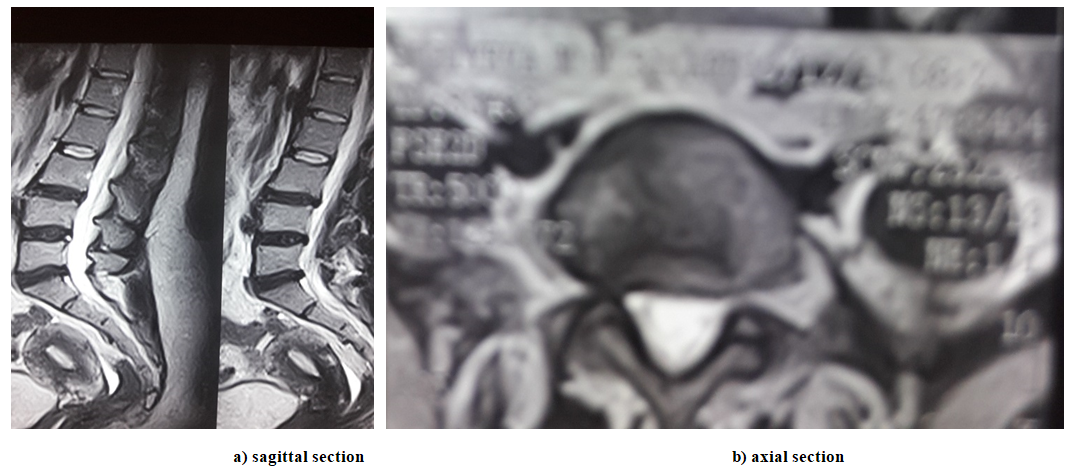
All patients who were admitted urgently had their neurological status assessed and MSCT performed./MRI of the lumbosacral spine to clarify the level, localization and nature of the pathological process (the level and localization of intervertebral disc involvement in the pathological process, the location of the intervertebral disc herniation across the spinal canal (median, paramedian, posterolateral or foraminal), the degree of herniation (elastic protrusion, sequestered prolapse).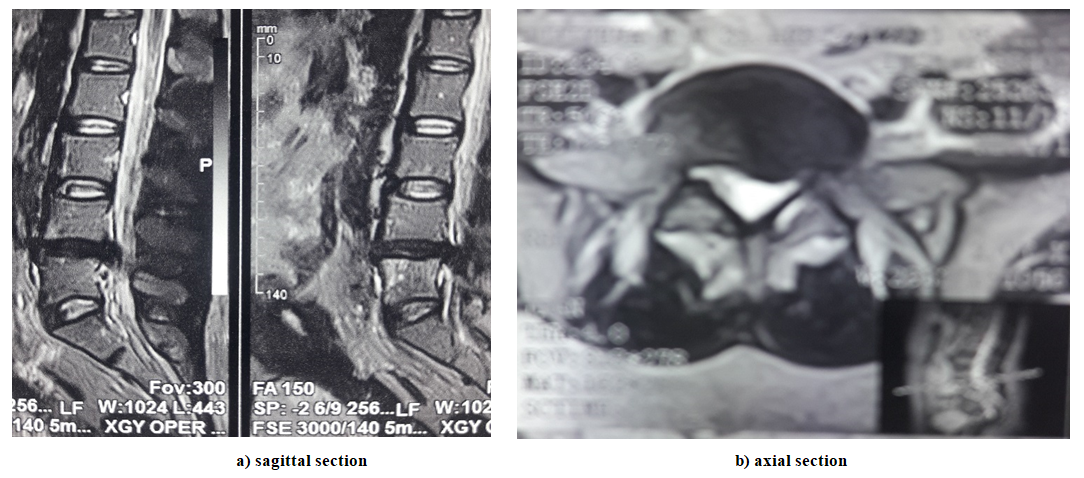 | Figure 2. MRI of a dislodged sequestered herniated intervertebral disc with migration of the fragment downwards at the vL4-L5 level |
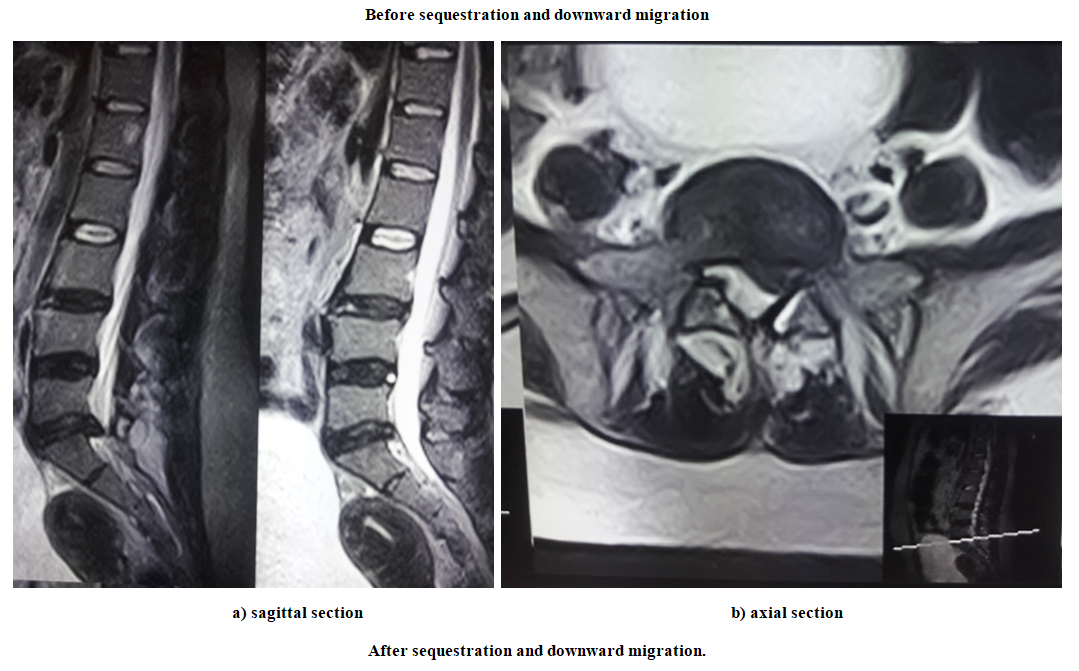
 | Figure 3. MRI of a dislodged sequestered herniated intervertebral disc with migration of the fragment downwards at the vL5-S1 level |
 | Figure 4 |
3. Results and Discussion
113 (95.8%) patients indicated the persistent nature of pain in the spine. Intermittent pain with minor physical activity or sitting was noted in 5 (4.2%) patients. 91 (77.1%) patients reported pain in both extremities. In 83 (70.3%) patients, the size of the hernial prolapse exceeded 10 mm across and migrated upward by more than 15 mm, in 35 (29.7%) patients, the size of the hernial sequester protrusion exceeded 10 mm across and migrated downward by more than 15 mm.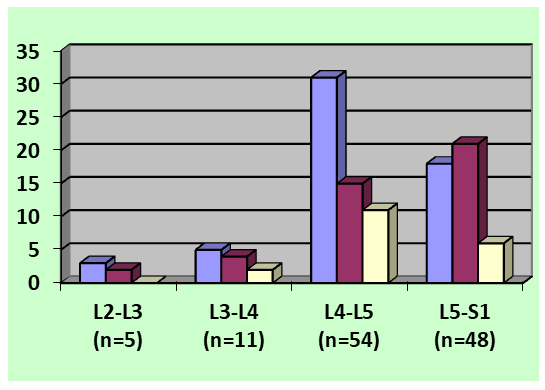 | Figure 5. Distribution of patients according to the level of localization of the intervertebral disc herniation and the direction of herniation protrusion |
All patients underwent surgery – interhemilaminectomy and ligamentectomy, L2-L3 (n=5), L3-L4 (n=11), L4-L5 (n=54) and L5-S1 (n=48) with removal of sequesters of the prolapsed disc, maximum lateral resection of the posterior wall of the radicular canal was performed in order to decompression of the dural funnel of the root outlet on the side of the predominance of radiculoischemia and radicular artery. Conservative treatment included analgesics, empirical antibiotic prophylaxis, anti-inflammatory, and vasoregulatory treatment. Iatrogenic paresis and paralysis, as well as expanded areas of sensitivity impairment were noted in 4 (3.4%) patients, and postoperative NSAIDs were observed in 18 (15.3%) cases. The most important category of vital activity - movement was significantly better restored in patients in the first group. In 92 (78.0%) patients in the postoperative period, NFTO completely regressed by the day of discharge, in the remaining patients it partially persisted until discharge. 11 (9.3%) patients retained lower mono- or paraparesis of varying severity, but strength in the extremities increased. Hypesthesia along the radiculoischemic root involved by compression persisted at the time of discharge in 28 (23.7%) patients.
4. Conclusions
Thus, our study revealed: 1. A common cause of radicular compression-ischemic syndrome (Cauda syndrome) is a giant herniated intervertebral disc that compresses several nerve roots. 2. As a rule, numbness of the urogenital region with impaired urination function and persistent pain in both or one leg is a manifestation of the recurrent syndrome of compression-ischemic radiculopathy. 3. The development of radicular compression-ischemic syndrome of discogenic genesis has a direct correlation between the frequency and timing of its development and the size and direction of migration of the hernia sequester. 4. Neuroimaging analysis made it possible to determine the level and localization of IVD herniation, anatomical relationships in the spinal canal, which were important when choosing the scope of surgical treatment. 5. Acute compression-ischemic radicular syndrome of discogenic genesis is a direct indication for emergency surgery, consisting in the removal of a herniated disc and decompression of the radicular canal. 6. The effectiveness of surgical intervention depends on the stage of radiclopathy of compression-ischemic genesis, the severity of neurological manifestations, the degree of compression of neurovascular formations, as well as on the timeliness of their full decompression.
References
| [1] | Biryuchkov Yu.V., Biryuchkov M.Yu. On the differentiated approach and technique of operations for compression syndromes of lumbosacral osteochondrosis. // Journal of Neurosurgery, 2006. Vol. No. 1, pp. 25-29. |
| [2] | Bogacheva L. A. Current state of the problem of back pain based on the materials of the 8th World Congress on Pain. Neurological Journal, 3, 1997, 59-63 |
| [3] | Bulgakov V., Lutsik A., Karpenko V., Epifantsev A.// Optimization of surgical treatment tactics in patients with lumbar osteochondrosis. Proceedings of the 4th Congress of Neurosurgeons of Russia. Moscow, 2006. - p. 18. |
| [4] | Golovko A.M., Baranovsky A.E., Shpakevich V.P. "Neurology and neurosurgery in Belarus". - №1 (01). - 2009.- Pp. 68-73. |
| [5] | Goryacheva M.V., Shumacher G.I., Malikov A.S., Dranitsa M.N., Sencheva N.A., Kuznetsova M.P., Polukhina I.P., Bondareva M.S. Correction of epidural venous blood flow disorders in patients with lumbar-sacral radiculopathy in the acute stage // Journal of MANUAL THERAPY.- 2012. - №3 (47). - Pp.14-18. |
| [6] | Gubenko I.A. Ponytail syndrome (Cauda syndrome). J. Neurology. - 2019. |
| [7] | Danilov V.I., Filatov B.C. Vertebrogenic compression lumbosacral radiculitis, radiculopathy (compressing factors and indications for surgical treatment). // Materials of the 3rd Congress of Neurosurgeons of Russia. St. Petersburg, 2002, pp.243. |
| [8] | Drivotinov B.V., Oleshkevich F.V., Karpenko E.A. Clinical, computed tomographic and myelographic characteristics of herniated lumbar intervertebral discs. the nerve. The System (Edited by I.P. Antonov). 1998. - Issue 21. - pp. 29-35. |
| [9] | Drivotinov B.V., Oleshkevich F.V., Karpenko E.A., Khodosovskaya V.M., Mikhailova G.I. Errors in the diagnosis of herniated discs and their clinical manifestations. // Actual problems of neurology and neurosurgery (Edited by A. F. Smeyanovich and I.P. Antonov) - 1999. - Issue 1. - pp. 46-56. |
| [10] | Zubairov E.Kh, Sak L.D. Endoscopic nucleotomy in lumbar disc surgery. Proceedings of the VII International Symposium "New technologies in neurosurgery". St. Petersburg: Man and Health, 2004, pp. 87-88. |
| [11] | Kariev M.Kh., Norov A.U., Ishmukhamedov S.N., Yugai I.A. Features of the clinical course of intervertebral disc herniations in degenerative lumbar stenosis //Vopr. neurosurgery. 2001. No. 3. pp.14-15. |
| [12] | Krivoshapkin, A.L. Herniated lumbar intervertebral disc: minimally invasive surgery and alternative locomotion / A.L. Krivoshapkin, A.D. Nekrasov, P.A. Semin; ed. by A.L. Krivoshapkin; GBOU VPO NGMU of the Ministry of Health of Russia. Novosibirsk: Academic Publishing house "Geo", 2014. 227 p. |
| [13] | Kushriruk P., Pisarev V. Anatomical and morphological justification of the use of medial facetectomy in microsurgical removal of herniated lumbar intervertebral discs // Proceedings of the IV Congress of Neurosurgeons of Russia - Moscow, 2006. P. 65. |
| [14] | Popelyansky Ya.Yu. Orthopedic neurology (vertebrology). A guide for doctors. 3rd edition revised and expanded. Moscow, Medpress-inform, 2003. |
| [15] | Popov B.C., Ivanov D.M. Endoscopic removal of lumbar disc herniations // Traumatology and orthopedics of the XXI century: collection of abstracts of the VIII Congress of Traumatologists-orthopedists of Russia. T. P. — Samara, 2006. -p. 731. |
| [16] | Bono CM, Garfin SR. History and evolution of disc replacement. / Spine J. 2004; 4: p. 145-150. |
| [17] | Boos N, Aebi M. Spinal Disorders: Fundamentals of Diagnosis and Treatment: Springer, 2008. |
| [18] | Davis R.A. // Journal of Neurosurgery. 1994. Vol. 80, N3. P. 415-421. |
| [19] | Hanley E. I., Howard B., Brighman C. et al. // Spine. 1994. Vol. 19, N18. P. 2122-2126. |
| [20] | Sprung C., Fabian A. Pitfalls in computed tomography of the cervical and lumbar spine/ Neurosurgical Review. 1994. Vol. 17, N1. P. 19-28. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML