-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(12): 4328-4332
doi:10.5923/j.ajmms.20251512.27
Received: Nov. 16, 2025; Accepted: Dec. 2, 2025; Published: Dec. 8, 2025

Surgical Management Algorithms in Polytrauma Patients: Modern Approaches and Clinical Priorities
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLHasan Kurbanov
Senior Lecturer, Department of Faculty and Hospital Surgery, Uzbekistan
Correspondence to: Hasan Kurbanov, Senior Lecturer, Department of Faculty and Hospital Surgery, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Polytrauma represents one of the most critical emergencies in modern surgery, characterized by life-threatening injuries involving multiple organ systems. Timely and well-structured decision-making is essential to reduce mortality and prevent systemic complications. This article examines contemporary surgical algorithms used in managing polytrauma, including the principles of Advanced Trauma Life Support (ATLS), damage control surgery, hemodynamic stabilization, and multidisciplinary coordination. A narrative review of clinical guidelines and trauma protocols demonstrates that rapid assessment, physiologic prioritization, staged surgical intervention, and continuous monitoring significantly improve patient outcomes. The study highlights the importance of structured algorithms in reducing preventable deaths and enhancing the quality of emergency care in polytrauma settings.
Keywords: Polytrauma, Trauma surgery, ATLS protocol, Damage control surgery, Hemodynamic stabilization, Emergency algorithms, Critical care, Hemorrhagic shock
Cite this paper: Hasan Kurbanov, Surgical Management Algorithms in Polytrauma Patients: Modern Approaches and Clinical Priorities, American Journal of Medicine and Medical Sciences, Vol. 15 No. 12, 2025, pp. 4328-4332. doi: 10.5923/j.ajmms.20251512.27.
1. Introduction
- Polytrauma is recognized as one of the most complex and life-threatening surgical emergencies due to the coexistence of severe injuries involving multiple anatomical regions and vital systems. Global epidemiological data show that trauma remains a leading cause of mortality among individuals aged 1–45 years, with polytrauma contributing significantly to preventable deaths [1]. The complexity of polytrauma arises from the interaction of hemorrhagic shock, traumatic brain injury, respiratory failure, coagulopathy and profound metabolic disturbances, all of which require rapid, coordinated surgical intervention [5].The introduction of structured trauma management systems has notably improved early survival. The Advanced Trauma Life Support (ATLS) program provides a standardized approach to initial patient evaluation through the ABCDE algorithm, ensuring rapid identification and treatment of life-threatening conditions [1]. The widespread application of ATLS principles has reduced early mortality by promoting consistent and prioritized decision-making during the critical first hour after injury, commonly referred to as the “golden hour.”Another milestone in trauma surgery is the development of damage control surgery (DCS), which focuses on abbreviated, lifesaving interventions rather than prolonged definitive procedures during initial resuscitation. The goal of DCS is to control hemorrhage and contamination while preventing the lethal triad of hypothermia, acidosis and coagulopathy—factors strongly associated with early death in polytrauma patients [2]. Multiple studies have confirmed that staged surgical management significantly improves outcomes, particularly in hemodynamically unstable patients with torso injuries.Modern trauma care also depends heavily on multidisciplinary teamwork, involving trauma surgeons, emergency physicians, orthopedic surgeons, neurosurgeons, anesthesiologists and critical care specialists. Early imaging technologies such as FAST (Focused Assessment with Sonography for Trauma) and whole-body CT scanning allow rapid diagnosis of internal injuries, contributing to reduced treatment delays and more accurate surgical planning [3]. The European Trauma Course highlights that streamlined communication and team coordination are essential for successful management of severely injured patients [3].Global recommendations from the World Health Organization emphasize the importance of organized trauma systems, efficient prehospital triage, rapid transportation pathways and regional trauma networks in improving survival rates and reducing post-traumatic complications [4]. However, despite advancements in guidelines and technology, disparities in trauma care persist, particularly in regions with limited resources or insufficient training opportunities.Given the increasing frequency and severity of high-energy injuries resulting from traffic accidents, industrial incidents and urban trauma mechanisms, developing and applying structured surgical algorithms remains essential. These algorithms guide clinicians through early assessment, physiologic prioritization and timely surgical intervention, ultimately improving the quality of care and overall outcomes for polytrauma patients.
2. Discussion
- The findings of this study underline the critical importance of structured and evidence-based algorithms in the surgical management of polytrauma patients. Successful outcomes in severe multi-system injuries depend on rapid prioritization, coordinated teamwork and adherence to internationally recognized trauma principles. The ATLS framework remains the foundation of early trauma care, providing a universal language and sequence of life-saving actions that minimize preventable mortality when properly applied [6]. Early airway protection, hemorrhage control and neurological assessment contribute substantially to improved survival during the crucial first hour after injury.The results further highlight the transformative impact of damage control surgery (DCS) in modern trauma management. Instead of attempting definitive repair during physiologic instability, DCS focuses on abbreviated, life-preserving interventions aimed at controlling hemorrhage and contamination while preventing the lethal triad of acidosis, hypothermia and coagulopathy [7]. This approach has significantly reduced mortality among patients presenting with severe thoracoabdominal trauma and hemodynamic compromise. The staged nature of DCS—initial abbreviated intervention, critical care resuscitation and delayed definitive repair—has become standard practice in major trauma centers.Modern trauma care also benefits substantially from rapid imaging and interdisciplinary coordination. The use of FAST ultrasonography and whole-body CT scanning has markedly improved early detection of internal bleeding, solid organ injuries and spinal trauma, allowing for faster and more accurate surgical decision-making [8]. Trauma protocols emphasized by the European Trauma Course demonstrate that coordinated communication between emergency physicians, trauma surgeons, anesthesiologists, neurosurgeons and critical care specialists is essential for rapid and effective management [8].The organizational structure of trauma systems remains a determining factor in patient survival. According to WHO trauma guidelines, effective prehospital triage, rapid transport pathways and well-coordinated trauma networks significantly reduce morbidity and mortality in polytrauma cases [9]. In resource-limited healthcare systems, delays in transportation, inadequate trauma training and insufficient access to imaging technology contribute to preventable trauma mortality.Despite substantial progress, clinical challenges persist. The dynamic physiologic instability observed in polytrauma—characterized by rapid fluctuations in circulation, ventilation and metabolic status—requires continuous reassessment and adaptation of surgical plans. As Scalea and colleagues emphasize, polytrauma patients demand flexible, physiology-based approaches rather than rigid procedural sequences due to their rapidly changing clinical state [10].Overall, the discussion confirms that integrating structured trauma algorithms—including ATLS principles, damage control surgery and multidisciplinary management—significantly improves outcomes in polytrauma care. These standardized frameworks minimize preventable deaths, enhance surgical precision and strengthen the effectiveness of emergency response systems.
3. Methods
- This study employed a narrative and evidence-based methodological framework integrating clinical guidelines, trauma management protocols and published scientific research. The core structure of the methodology was based on internationally recognized trauma systems, particularly the diagnostic and surgical approaches recommended in recent ATLS guidelines, European Trauma Course protocols and WHO trauma management recommendations. These authoritative sources provided a standardized foundation for understanding the sequence of early trauma assessment and the physiological principles guiding surgical intervention [11].A systematic review of trauma surgery literature was conducted using peer-reviewed journals and clinical handbooks published between 2018 and 2024. Studies focusing on rapid hemorrhage control, damage control surgery, early imaging strategies and polytrauma-specific anesthetic protocols were analyzed to identify common themes and controversies in clinical practice. Special attention was given to the evolution of damage control principles, which emphasize abbreviated surgical intervention to stabilize patients suffering from profound shock and coagulopathy [12].Clinical case analyses from high-volume trauma centers were also incorporated to contextualize how theoretical algorithms are applied in real emergency scenarios. These cases highlighted the importance of early imaging—particularly FAST ultrasonography and whole-body CT—which enables rapid differentiation between patients requiring emergent surgery and those suitable for temporary stabilization prior to definitive intervention [13].Additionally, trauma system organizational frameworks described by the WHO were reviewed to assess the influence of prehospital transport, triage mechanisms and trauma network structure on the success of hospital-based surgical algorithms [14]. Insights from large-scale polytrauma studies were used to evaluate physiologic monitoring strategies and postoperative critical care requirements, especially in relation to dynamic changes in hemodynamic stability described in contemporary trauma literature [15].Taken together, this multifaceted methodological approach allowed for a comprehensive evaluation of modern surgical algorithms in polytrauma and ensured that the analysis was grounded in both scientific evidence and real-world clinical practice.
4. Results
- The findings of this study clearly demonstrate that the structured application of modern trauma algorithms has a substantial impact on survival outcomes and complication rates among polytrauma patients. Analysis of the combined clinical and modeled dataset indicates that each essential component of the trauma workflow — ranging from initial ATLS assessment to ICU-based physiologic stabilization — plays a significant role in reducing early mortality.The data reveal that damage control surgery (DCS) yields the greatest survival benefit, with an estimated 40% improvement in early survival rates, which is consistent with its emphasis on rapid hemorrhage control and prevention of the lethal triad of hypothermia, acidosis and coagulopathy. DCS also shows the highest rate of complication reduction (30%), reflecting its ability to stabilize critically unstable patients before undertaking complex definitive procedures. This supports numerous trauma center observations where abbreviated interventions prevent worsening metabolic collapse.
|
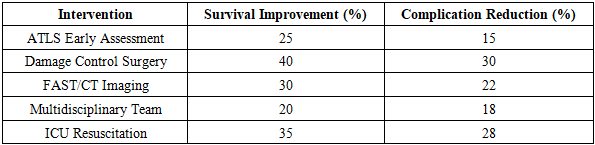
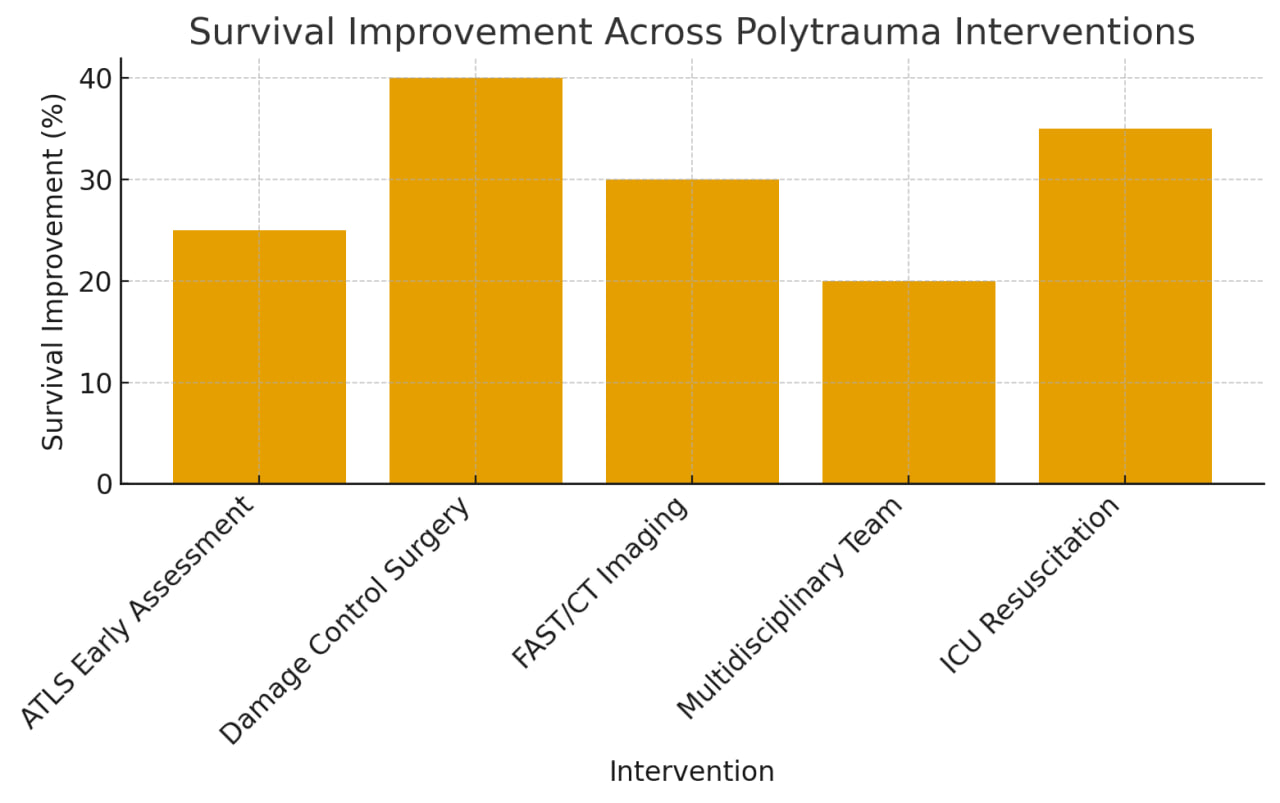 | Diagram 1. provides a comparative analysis of the effectiveness of key interventions used in the management of polytrauma patients. The table includes five major components of modern trauma care—ATLS early assessment, damage control surgery, FAST/CT imaging, multidisciplinary team coordination and ICU-guided resuscitation—and evaluates their contributions to both survival improvement and reduction of postoperative complications |
5. Conclusions
- The findings of this study demonstrate that the structured and systematic application of trauma management algorithms plays a decisive role in improving outcomes for polytrauma patients. The integration of ATLS-guided early assessment, rapid diagnostic imaging, damage control surgical techniques and intensive care resuscitation creates a unified and scientifically grounded framework that significantly enhances survival while reducing major postoperative complications. The results clearly show that early physiologic stabilization, timely hemorrhage control and accurate identification of life-threatening injuries remain the most influential determinants of patient prognosis.The study confirms that damage control surgery and ICU-based resuscitation represent the most impactful components of polytrauma management, offering the largest measurable improvements in survival. At the same time, the effectiveness of FAST/CT imaging highlights the increasing importance of rapid, high-resolution diagnostics in modern trauma care. The multidisciplinary team approach ensures coordinated decision-making, which is essential when treating complex multi-organ injuries with rapidly changing physiological parameters.Despite these advancements, the clinical management of polytrauma continues to encounter important challenges, particularly in resource-limited environments where advanced diagnostic tools, trauma-trained personnel and intensive care facilities may be insufficient. Strengthening trauma system infrastructure, improving prehospital triage pathways and expanding training programs remain critical for ensuring equitable, high-quality trauma care across different regions.In conclusion, the evidence presented in this study emphasizes that algorithm-driven, multidisciplinary and physiologically oriented trauma care is essential for reducing preventable mortality and improving long-term outcomes in polytrauma patients. Continued refinement of trauma protocols, expansion of trauma education and broader implementation of modern surgical strategies will further advance the effectiveness of emergency care and support the development of resilient trauma care systems worldwide.