-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(12): 4298-4306
doi:10.5923/j.ajmms.20251512.21
Received: Nov. 3, 2025; Accepted: Dec. 1, 2025; Published: Dec. 8, 2025

Stages of Burnout Syndrome Among Professionals in Various Fields
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLYadgarova Nargiza Faxritdinovna1, Kevorkova Marina Anatolevna2
1PhD, Associate Professor, Department of Psychiatry and Narcology, Tashkent State Medicine University, Tashkent, Uzbekistan
2PhD, Senior Lecturer, Department of Psychiatry and Narcology, Tashkent State Medicine University, Tashkent, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Burnout Syndrome is a psychological condition affecting healthcare professionals, primarily due to high workloads, prolonged patient interactions, and emotional strain. This study aimed to assess burnout levels among physicians in different medical fields and identify factors contributing to its severity. Materials and methods. An observational study was conducted among 208 physicians at medical institutions in Uzbekistan. Participants were divided into two groups: general practitioners (n=173,83.1%) and specialists (n=35,16.9%). Burnout levels were evaluated using the Maslach Burnout Inventory, Boyko’s Emotional Burnout questionnaire, and a specialized rating scale. Burnout prevalence was analyzed based on years of experience, workload, and professional responsibilities. Results. The findings revealed that general practitioners had a significantly higher prevalence of burnout (48.5%) compared to specialists (28.8%). Moderate burnout was more frequent among specialists (32.1%) than among general practitioners (24.6%). Burnout severity increased with years of experience, workload, and responsibility, leading to emotional exhaustion, professional detachment, and reduced motivation. Conclusions. The study highlights the urgent need for psychological support, improved working conditions, and stress management strategies to reduce burnout among physicians. Targeted interventions are necessary to preserve mental well-being and ensure high-quality patient care.
Keywords: Burnout syndrome, Emotional exhaustion, Professional competence, Maslach Burnout Inventory, Stress resilience
Cite this paper: Yadgarova Nargiza Faxritdinovna, Kevorkova Marina Anatolevna, Stages of Burnout Syndrome Among Professionals in Various Fields, American Journal of Medicine and Medical Sciences, Vol. 15 No. 12, 2025, pp. 4298-4306. doi: 10.5923/j.ajmms.20251512.21.
1. Introduction
- Burnout syndrome (BS) remains one of the most significant occupational health challenges of the modern era, particularly among healthcare professionals. The World Health Organization [26] defines burnout as an occupational phenomenon resulting from chronic workplace stress that has not been successfully managed. It manifests through three primary dimensions: emotional exhaustion, depersonalization, and reduced personal accomplishment [14]. These dimensions collectively reflect the progressive depletion of emotional and physical energy under continuous professional strain. Over the past five years, research on burnout has intensified due to the COVID-19 pandemic, which has drastically altered the landscape of healthcare delivery worldwide. According to recent meta-analyses [5,7], burnout prevalence among healthcare professionals post-pandemic ranges between 45% and 68%, with significant variations across specialties, countries, and healthcare systems. Factors contributing to this increase include prolonged exposure to patient suffering, increased workload, and limited institutional support. Studies in Asia and Eastern Europe [10,19] also indicate that physicians in resource-limited settings experience heightened levels of emotional exhaustion due to workforce shortages and administrative burdens.In Uzbekistan the problem of physician burnout has been under-investigated despite its evident clinical and social relevance. Local physicians often face excessive workload, low remuneration, and minimal access to psychological assistance or rest facilities, all of which contribute to burnout. Previous regional studies [1,13] have highlighted the urgent need for developing preventive and rehabilitative interventions that address both organizational and personal resilience factors. The theoretical understanding of burnout has evolved through multiple frameworks. The Job Demand-Resources (JD-R) model [3] conceptualizes burnout as the outcome of chronic imbalance between professional demands and available resources. When job demands – such as workload, cognitive strain, and emotional labor-exceed resources like autonomy, feedback, and social support, individuals develop exhaustion and disengagement. Similarly, the Conservation of Resources (COR) theory [9] explains that stress occurs when individuals perceive a threat to their personal resources (e.g., time, emotional stability, or energy) and lack mechanisms for their recovery. Modern interpretations integrate these frameworks to account for cultural, technological, and systemic influences on burnout, particularly in healthcare.Recent empirical research [8,16,22] underscores that burnout is not merely an individual problem but a systemic outcome of healthcare design. High administrative workload, digital documentation overload, and poor work–life integration are consistent predictors of physician exhaustion. The 2025 Lancet Digital Health report [12] also demonstrated that the introduction of artificial intelligence and digital assistance systems reduces burnout risk by streamlining administrative duties and improving efficiency. However, such technological support remains scarce in low- and middle-income countries, where healthcare systems rely heavily on human labor and traditional management models.Post-pandemic analyses [7,21] reveal a shift from acute stress during the crisis phase to chronic fatigue, moral distress, and depersonalization in the recovery period. Physicians working in primary care and emergency medicine continue to report higher burnout rates compared to specialists in non-acute disciplines. General practitioners face unique stressors such as patient overload, emotional labor, and inadequate recovery time [19]. These findings are consistent with earlier global studies [17,25], which emphasize that sustained emotional exhaustion leads to decreased empathy, professional detachment, and reduced patient safety.Gender, age, and professional experience also influence burnout severity. Female physicians, especially those balancing professional and family roles, show higher susceptibility to emotional exhaustion [2,18]. Younger clinicians report frustration due to limited career autonomy, while senior doctors face chronic fatigue related to long-term stress accumulation [10,23]. Organizational factors such as leadership quality, peer support, and institutional culture significantly mediate burnout outcomes [6]. Addressing these determinants requires a systemic approach integrating psychological support, institutional reforms, and policy-level strategies for physician well-being.Given this background, the present study aims to assess the prevalence and severity of burnout among physicians across various medical disciplines in Uzbekistan, to identify its key determinants, and to provide recommendations for prevention and rehabilitation. The novelty of this work lies in its regional focus, examining burnout within a transitional healthcare system adapting to global post-pandemic challenges. By situating local findings within the broader international discourse, this research seeks to contribute to the growing body of literature advocating evidence-based interventions, technological innovation, and institutional reform to mitigate burnout and enhance professional resilience.
2. Materials and Methods
- Study population. In total, 208 physicians participated in the study. The study was conducted in a clinical trial format involving two groups. The first group (study group) comprised 83.1% (n=173) of general practitioners, while the second group (control group) included 16.9% (n=35) of specialists from narrow medical fields – neurologists, infectious disease specialists, obstetrician-gynaecologists, psychiatrists, as well as addiction specialists . Both groups of respondents were assessed using the same methodology. Physicians aged between 27 and 59 years participated in the study. The average age of respondents in the first group was 35.9±0.85 years, while in the second group, it was 31.5±0.24 years. Physicians with work experience ranging from one month to 39 years were evaluated. In terms of work experience, the average professional experience in the first group was 18.04±24.12 years, whereas in the second group it accounted for 20.09±27.02 years. To achieve the research objectives, a modified version of the Maslach Burnout Inventory (MBI) for medical professionals by K. Maslach and N.V. Vodopyanova [14,24] was used, along with V.V. Boyko’s "Emotional Burnout" questionnaire [4] and a specially developed rating scale. All study participants were diagnosed according to the ICD-10 classification under the F-40 category for stress-related and somatoform neurotic disorders.
3. Results
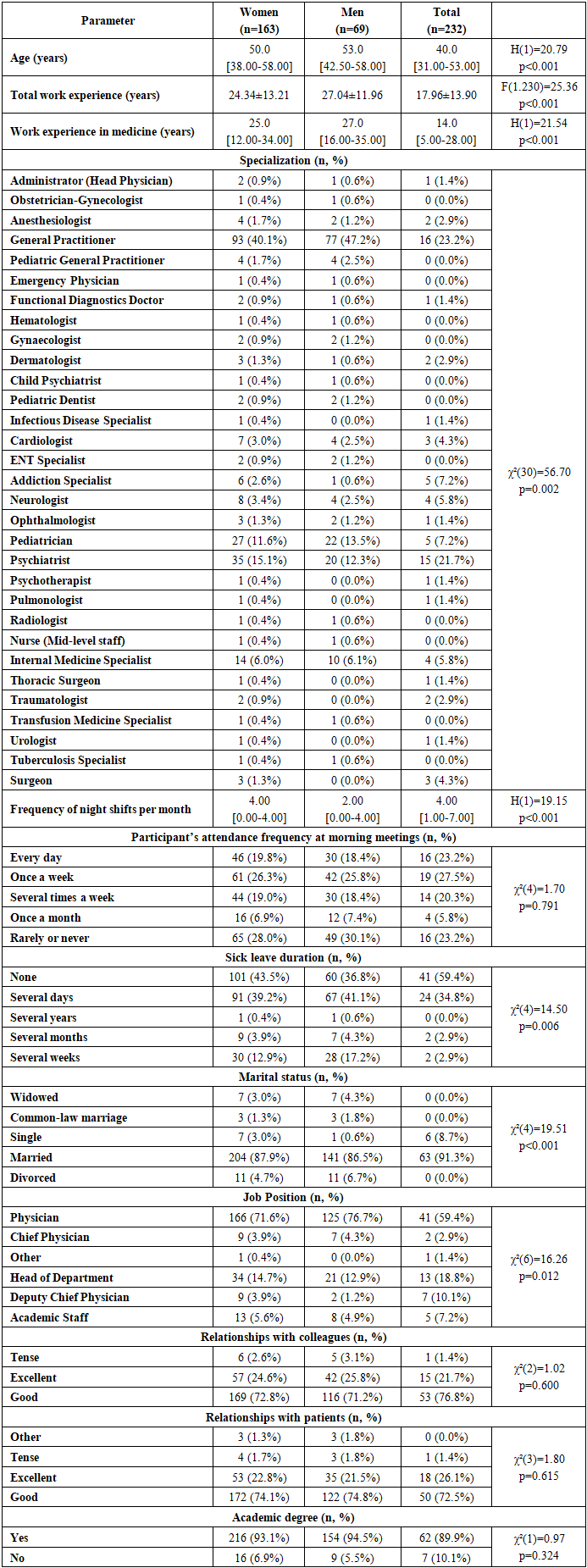
- The study included 232 medical professionals, of whom 163 (70.3%) were women and 69 (29.7%) were men. The age of participants ranged from 31 to 58 years, with a median age of 50 years for women and 53 years for men, correspondingly. Male participants appeared to be significantly older than females (H=20.79, p<0.001).
|
|
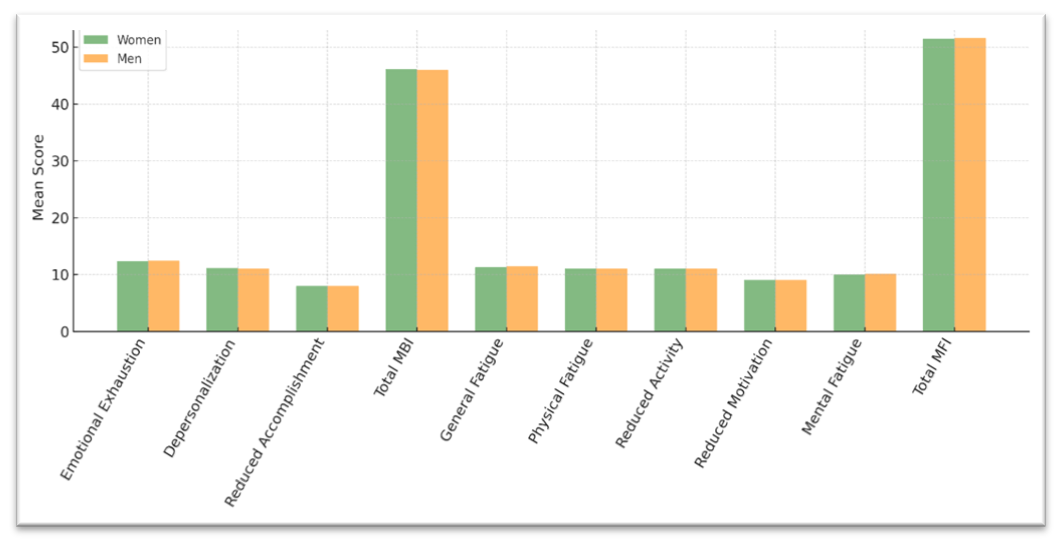 | Figure 1. Comparison of burnout Fatigue indicators by gender (MBI and MFI-20) |
|
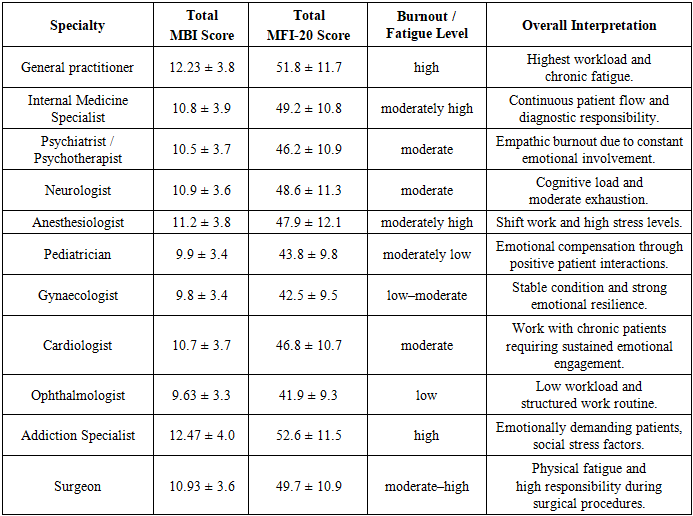
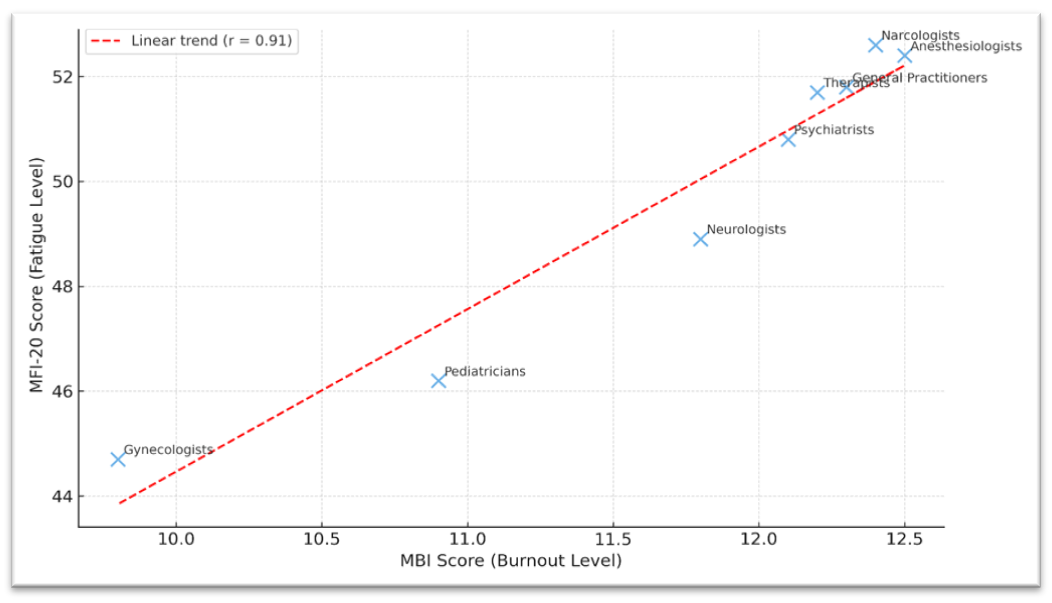 | Figure 2. Correlation between burnout levels (MBI) and fatigue levels (MFI-20) among physicians of different specialties |
4. Discussion
- One of the most striking patterns revealed was the correlation between years of professional experience and burnout severity. Physicians with more than 20 years of experience exhibited the highest levels of emotional exhaustion and depersonalization, indicating a cumulative stress effect. Similar observations have been made by West et al. [25] and Fujimori et al. [7], who found that prolonged exposure to high emotional demand without adequate recovery increases physiological and psychological vulnerability. The results suggest that long-term service in emotionally charged clinical environments leads to progressive depletion of coping resources. Consequently, sustained professional exposure without periodic psychological support or balanced workload redistribution may allow routine occupational stress to evolve into chronic burnout. These findings emphasize the necessity for longitudinal monitoring of experienced physicians and for integrating preventive measures such as sabbaticals, rotation schedules, and targeted stress-reduction programs.Daily exposure to high patient volumes, administrative demands, and inadequate recovery time were the primary contributors to emotional exhaustion. In contrast, specialists, although generally reporting lower burnout rates, showed moderate levels of depersonalization and reduced personal accomplishment, particularly in intensive care, oncology, and obstetrics. These results are comparable to those of Shanafelt et al. [21], who emphasized that prolonged involvement in emotionally demanding patient care leads to a loss of empathy and diminished sense of professional fulfillment. The contrast between generalists and specialists underlines that the frequency and diversity of patient interactions may be more stressful than the clinical complexity itself. Therefore, developing effective scheduling systems, administrative assistance, and emotional-support frameworks for primary-care physicians becomes critical for mitigating burnout.The study also highlighted gender and age-related differences. Female physicians demonstrated slightly higher emotional exhaustion scores than males, a finding consistent with Alonso et al. [2] and Garcia et al. [8], who noted that female clinicians often experience additional psychosocial strain related to work–family balance and cultural expectations. Younger physicians exhibited elevated stress due to limited autonomy and professional insecurity, whereas senior clinicians manifested chronic fatigue accumulated over years of service. These patterns show that burnout determinants evolve across the professional lifespan. Tailored prevention strategies should therefore account for both generational and gender-specific needs: mentorship and skill-development programs for younger physicians, flexible scheduling and family-friendly policies for women, and restorative interventions for senior staff experiencing cumulative fatigue. In addition, the results reaffirm the importance of organizational and psychosocial factors. Lack of institutional support, poor communication with administration, and limited access to psychological counseling were frequently reported among respondents. These observations align with data from the WHO [26] and Dzau et al. [6], which stress the necessity of structural interventions rather than relying solely on individual coping strategies. Hospitals with integrated well-being programs, regular supervision, and peer-support systems demonstrate significantly lower burnout levels among staff. Organizational culture that encourages open communication, fair workload distribution, and recognition of professional achievements can serve as a powerful protective factor. Therefore, systemic reform should accompany individual-level interventions to achieve sustainable improvements in physicians’ mental health.Interestingly, a subset of specialists – particularly those in neurology, psychiatry, and gynecology – displayed high depersonalization levels despite moderate overall burnout scores. This may reflect emotional detachment as a protective mechanism, a pattern described in Hobfoll’s [9] Conservation of Resources theory. Emotional distancing helps maintain professional functioning but may, over time, impair empathy and job satisfaction. Therefore, early psychological support and structured peer discussions should be encouraged to transform adaptive distancing into healthy professional boundaries. Continuous education in emotional regulation, supervision meetings, and reflective practice groups can prevent depersonalization from progressing to full burnout and maintain high standards of patient care.Another notable observation concerns the role of post-pandemic adaptation. Physicians who had direct experience treating COVID-19 patients reported persistent fatigue and decreased motivation, even several years after the pandemic. This chronic post-stress fatigue mirrors international findings [5,16] that identify COVID-related moral injury as a long-term burnout determinant. The persistence of such symptoms underscores the need for specialized rehabilitation programs focused on trauma recovery, moral distress counseling, and restoration of professional confidence. Post-pandemic mental-health initiatives should be incorporated into occupational-health frameworks to ensure ongoing monitoring and support of healthcare workers exposed to crisis conditions.Overall, the results confirm that burnout in the Uzbek medical context shares many features with global trends, while also being influenced by local systemic challenges – such as limited institutional support, administrative overload, and insufficient psychological services. The lack of preventive interventions exacerbates vulnerability to chronic exhaustion. Introducing systematic stress management training, mentorship programs, and professional supervision could substantially mitigate burnout rates [11]. National-level strategies should prioritize physician well-being, integrating psychological services into primary-care settings and ensuring funding for continuous education on resilience and self-care.From a clinical standpoint, burnout among physicians not only affects mental health but also has practical implications for healthcare outcomes. Emotional exhaustion leads to increased diagnostic errors, reduced empathy, and diminished patient satisfaction [17,20]. Consequently, addressing physician burnout should be recognized as a public health priority. Interventions should include early detection using validated scales such as the Maslach Burnout Inventory (MBI) and Boyko’s “Emotional Burnout” questionnaire, continuous mental-health screening, and targeted counseling. Incorporating wellness metrics into institutional performance indicators can further enhance accountability and encourage hospitals to invest in workforce well-being.In conclusion, the findings of this study emphasize the multidimensional nature of burnout syndrome among healthcare professionals in Uzbekistan. The higher burnout prevalence among general practitioners highlights the need for immediate systemic and psychological interventions. Comparative analysis with international data supports the view that burnout represents not merely an individual issue but a collective institutional and societal challenge. Comprehensive reforms focusing on workload optimization, administrative simplification, leadership training, and continuous psychological support can improve both physician well-being and quality of patient care.
5. Conclusions
- The present study demonstrates that emotional burnout and professional fatigue are significant and prevalent issues among physicians of various specialties. The most vulnerable groups were those exposed to intense emotional demands and heavy patient flows, particularly primary care physicians and addiction specialists. The strong association observed between emotional burnout and fatigue highlights the need for a comprehensive prevention strategy that includes workload optimization, psychological support, and regular monitoring of healthcare workers’ emotional well-being. These findings indicate that burnout should be viewed not only as an individual response to stress but also as an indicator of organizational functioning. Effective prevention requires systemic changes aimed at improving working conditions, rational distribution of professional responsibilities, and fostering a corporate culture that prioritizes the emotional well-being of medical staff.